
Transformation into the Vermont Butterwolf!


Transformation into the Vermont Butterwolf!
Some amazing musings on Borderline Personality “disorder” by taking the mask off. Beautiful post. I will comment later.
Later: one comment i did want to make is this: so far as i know, and despite current claims, RW never claimed to suffer from anything other than depression and drug and alcohol addiction. He never to my knowledge claimed to be “bipolar.” Now, if one of his drugs of choice in self-medicating his depression was cocaine, and i am not saying i know this to be a fact, only supposition, then that RW may have been using also Alcohol to reduce the manic frenetic highs of cocaine, not that he naturally experienced highs and lows.
But now certain website want to place Williams under their bipolar umbrella.
I frankly find it troubling this push to subsume everyone with depression under t he bipolar blanket.
If it produced fewer people suffering from longterm disability and mental illness as a result, then i would cheer it. But in point of fact, research has shown that even in strictly diagnosed Bipolar 1 in which mania, naturally has occurred, treatment with lithium has not in fact served people as well as they claim. In decades before lithium came on the market, before they claimed to be able to “treat” manic-deproession, sufferers largely were rarely seen in the large state hospitals and usually only on a temporary basis. They were not longterm or chronic patients. Usually they got better and if they occasionally suffered downs again, the manic episodes might never be seen again after the initial one. The point being that bipolar susceptibility was not the chronic and terribly disabling illness that it has suddenly become, and i blame the medications for that development. That and the huge expansion of the diagnosis into BipolarII so that everyone with depression, even bereavement, is now labelled bipolar with several devastating consequences.
one is that the person is told they have a chronic, severe incurable mental illness for which they must take meds the rest of their lives, which will end up being a vicious cycle. That mentality produces enormous disability, lifelong. Two is that it ruins lives that might have been productive had the verdict been less dire and the treatment less dire too. Instead of telling someone who is depressed that their occasionally periods of cheer or even anger are appropriate, doctors see them as symptoms of this new entity bipolar II and use new useless drugs on them, including antipsychotics, with terrible side effects and psychological effects that are even worse. I have literally never seen anyone once diagnosed with Bipolar II get better unless they rejected the dx entirely and left the labeling System altogether…how can anyone escape it otherwiThey want you to believe that your moods are an illnesss rather than a healthy way to fight back against depression, as if it is abnormal to feel anything other than sadness! It is, in a word Meshugas of the highest order.
This is from the New York Times today:
To the Editor:
Re “When Cell Door Opens, Tough Tactics and Risk” (“Locked In” series, front page, July 29):
The events leading to Charles Jason Toll’s death highlight the dangers of prison procedures, especially for vulnerable inmates who suffer from mental illness. Particularly concerning is Mr. Toll’s solitary confinement, a disciplinary technique repeatedly identified as ineffective and counterproductive, and even as torture.
The Justice Department has found that solitary confinement of mentally ill people violates their rights under the Eighth Amendment and the Americans With Disabilities Act.
Solitary confinement worsens psychological symptoms and can trigger outbursts tied to the person’s feelings of hopelessness and loss of a sense of self through extreme social isolation and sensory deprivation.
Providing mentally ill people with appropriate and compassionate mental health care, including integration of psychiatric, psychological and psychoanalytically oriented treatments, is crucial in restoring a person’s identity, alleviating feelings of loss and distress and reducing violence.
Mr. Toll’s solitary confinement, suffering and death were avoidable, and again show that the mentally ill are more likely victims of violence, not the perpetrators.
SUSAN McNAMARA
Middletown, Conn., July 30, 2014
The writer is a psychiatrist.
_____________________________
When I was a patient in May and June 2014 at New Britain’s Hospital of Central Connecticut, Dr Michael Edward Balkunas regularly imprisoned me in a horrific seclusion cell, without a single amenity but a concrete built-in bed and rubberized mattress, for nothing more than making too much noise for the approved hospital milieu. In fact, several nurses took it upon themselves, with Dr Balkunas approval, to do the same. This became literally routine. I was NOT, as is required by the Centers for Medicare and Medicaid, in IMMINENT danger of causing severe harm to myself or others. No, I was loud, disruptive and uncooperative, and I was rude. Period.
My first reaction when the double doors locked behind me was immediately to start screaming, at the top of my lungs, from the base of my lungs. But screaming brought no one. Okay, they did soon come in at me with three IM injections, but they came back every time with IM injections anyway, because as I took to calling it, these were part of the drill, they were “punishment injections.” I was pushed onto my stomach and shoved into the mattress so I couldn’t breathe and injected whether I liked it or not. I tried to say, “STOP! I will take the injections, just don’t hold me down.”
But sometimes they didn’t listen to me, and held me down anyway, and I got scared that they would kill me, because it didn’t matter that I didn’t struggle. There were four of them to the one of me, and they expected me to fight and so they forced my face into the mattress and held me tight, hard, and with all their weight….until I felt my breath go out of me. Did they have any idea that I was NOT struggling, that I felt I was going to die? Did they have any idea that they were killing me?
I don’t know. I don’t know. All I know is that I felt in mortal danger when they wouldn’t let me just accept the injections on my own, in my arm, but insisted on giving them to me by force in the buttocks, even when I said I would take them voluntarily.
Then they would leave and lock the double doors. And I would scream, and NO ONE would respond, even though I eventually learned that they could not only hear me through the intercom hidden somewhere in the ceiling, they could also talk to me. They wouldn’t but they could have. When screaming brought no one, I would strip and urinate on the floor, and I would defecate too as much as i could, and smear everything on the walls and floor. I would even eat it and paint it on my body. I didn’t care, I DIDN’T CARE! I just wanted someone to come in and help me.
Several times I washed and colored my hair with urine, thoroughly. But no one came back for hours. The urine, which completely soaked my hair, had time to dry completely. Not that they cared or noticed. If they had, they said nothing. It was nothing to them. Only Barbara RN asked me what was in my hair, and insisted that she wash it out when finally they released me. I went with her to the shower-tub room and allowed her to do so, but only one other person was kind enough to notice and do that. Everyone else just released me and expected me to somehow be reformed and “better” after my hours of punishment.
Of course that wasn’t the case. I got worse, much worse. I started defecating in my bedroom, at any hour,for any reason, any time I was frustrated or angry. They decided I had “borderline personality disorder,” that I was simply manipulating them. They failed to see that they had traumatized and broken me. They failed to see their continuing role in my behaviors…which were getting worse and worse the more they punished me. Every time they secluded me, or four-pointed me, I regressed more.
Dr Balkunas actually decided to commit me to the State Hospital claiming it would help me “get better.” But really he was just in punishment mode. You could tell, because he wasn’t using any of the methods that you are supposed to use for REAL borderline patients….If he really believed I was BPD he wouldn’t have kept at it. But he knew from my brother, a psychiatrist too, and my own psychiatrist, that I do not have BPD, so that was bogus and just an excuse to torture me. He didn’t really think I had BPD. He just needed an excuse to use solitary confinement and he knew that schizophrenia was NOT a good reason. A very BAD reason in fact, so he invented a secondary diagnosis to use. But the thing is, there are other therapies you are supposed to use in BPD, and he never bothered to treat me with anything but punishment and then threw up his hands and said, Well, the antipsychotic drugs take time to work, so you will go to the SH until they do.
Bastard! He gave up on me without even trying to help…so-called saintly doctor. Just a bastard! Because torture doesn’t work to make me better, he decides that I am the one at fault????? Well GO FUCK HIM UP THE ASS WITH A BROKEN GLASS JAR!
I figured this out while living alone. I would panic when I felt myself choking. It works like a miracle, because it is usually a spasm in the upper throat, near your mouth, and not a closed off pharynx that causes coking sensationss. You just have to understand that you CAN still breathe through your nose and that will end the panic. Once the panicky feelings are over, everything is easier to deal with and you can usually spit out the food or even find a way to swallow it. But at least you realize that you are not imminently going to die, which is a good thing to know.
Hope this advice helps someone. If it does, I would love some feedback. I have offered it to friends, and they have loved it, found it useful too, so I know it works.
Best wishes to all,
Pam
Actually I “deserved” four-point restraints. I was “violent.”

But I want to explain what “deserving” restraints and being “violent” at New Britain General Hospital (Hospital of Central Connecticut) means in 2014.
I also want to tell you something else even more important: In Connecticut, the staff at almost every psychiatric unit or hospital will insist that “we only use seclusion and restraints when essential, when a patient is absolutely out of control and extremely violent, and cannot be controlled in any other way.”
Trust me, I know, because they have said this to me.
But what you need to know is that they are NOT talking about some 300 pound man hopped up on PCP, waving a machete. For one thing, that person, whom I believe to be largely mythical at least in ordinary psych units, or if real now largely confined to correctional and law enforcement settings, the person they are talking about, the rule, not the exception to the rule of the “extremely violent” person whom they claim must be restrained due to lack of any other method of control, is, to put it grammatically correctly, I.
And let me tell you about me. I will turn 62 years of age in November. I am 5 feet 3 inches tall, weigh, maybe 110 pounds on a good day, and have been consistently described as “poorly muscled.” I am also unable to use my left arm for much of anything, due to injuries sustained at the Institute of Living in 2013, including a small tear in my rotator cuff and possibly more than that– a fact the HOCC nurses/security guards knew and used to their advantage when subduing me. I also want you to know that I am a decades-long vegetarian on the principle of non-violence — to people as well as to animals. I have opposed the death penalty since I was a nine year old child (when I first learned of it) and do not even believe in the principle of prisons, or in treating our convicted “criminals” the way we do now.
Yet in every single hospital I have been in since 2000, and of course for years before then (“before they knew better”) I have been brutally secluded and restrained multiple times as “OOC” — out of control — and “violent.” In addition to either physically holding me down by brute force, one person to each limb and one to my torso (this was at the only 2 hospitals that did not actually resort to mechanical four-point restraints– compared to the dozen others that did), they would routinely inject me with one to three drugs as chemical restraints.
I am the rule, not the exception to it, of their supposedly “extremely violent mental patient” who is so OOC — out of control — that Connecticut hospitals refuse to eliminate the use of restraints and seclusion, because they “might need them.” I am the typical example of the person they claim they absolutely must have the right to resort to violence against, for their own safety and mine.
Okay, so am I truly violent? What did I do to deserve their brutality? Or should we say, their “protective measures?” Well, at HOCC, in the Emergency Department, this is what happened, and I kid you not: I came in by ambulance, involuntarily, in the sense that I did not want to go but was brought in by EMTs and given the “either the easy way or the hard way” choice by police. But I did not resist it or fight. I was not restrained in the ambulance. in fact, I was mute and merely handed them my med sheet and my detailed Advanced Directive, on the first 2 pages of which is the important information about my trauma history and the critical need to know points about how to deal with me.
When I arrived I was quickly shunted to the psychiatric crisis section and into a curtained off cubicle. No one took my cell phone from me, or the single book of my artwork that I had managed to bring with me. So I texted everyone I could for as long as I could. For a while I tried to obtain a crayon to communicate with, eventually and in desperation, writing with ketchup on the outer carton of my dinner container, begging for something to write with. Instead of helping me out, the head ER nurse penned me a note saying that I would not get anything to write with, that either I spoke out loud or she would not listen to me. How very odd and evil that she wrote this to me! She didn’t speak to me, she wrote it, as if I were deaf, even while saying that she knew I could speak and would not talk with me unless I did so… The idiocy of that act just sends sparks of rage through my brain even now. She later spied my art book next to me on the gurney, and suddenly rushed me, snatched it out from under my thigh and raced away with it, holding it triumphantly as if she had won a prize. I was incensed. Why hadn’t she just asked me for it? And how did I know what she was going to do with it? Would she keep it safe and sound? Actually, though, I mostly just reacted instinctively: Someone had stolen the only thing I had of my own in my possession, and she had simply snatched it away from me, without a word or even a polite request. So I did as anyone would do, I think. I raced up behind her and snatched it back! Well, that was a mistake. That was bad, that was bad bad bad. I heard people groan and swear. I was grabbed from behind by two security guards and the book was wrenched from me again.
Remember, I was mute so I couldn’t say anything, but I tried to resist, tried to gesture that the book was mine and she had no right too take it from me. Instead of explaining that she would protect it and take care of my things, people started talking about how I had attacked the nurse, had assaulted her…She told them to put me in seclusion. The guards dragged me, resisting in panic, towards this hidden room, and I heard another nurse warn them of my medical history with a torn left rotator cuff. Hearing this, the guard on my left side, grabbed my shoulder and wrenched it higher until I let out a blood curdling scream, wordless but vocal. “Aha! I thought you could make sounds!” he said in triumph, wrenching me again until I sobbed in agony. Then they dumped me in the seclusion room, with only a hospital johnnie on me, and locked the door behind them.
Even though I had no words to speak my rage and panic, I screamed and screamed. They came through the door with needles, held me down and injected me. Then, when in a rage reaction, I disrobed, they decided to four-point restrain me. I heard a guard say, “we really have no reason to restrain her, you know.” But the other said, “It doesn’t matter, we will find a reason.” So they did . Terrified, I did not resist, because they held me down by the left shoulder causing me so much pain I was afraid they would hurt me permanently. I also hoped upon hope that if I didn’t resist, they would let me out quickly. Believe me, I had been through this routine enough to know what to try to do to minimize the consequences and the damage…
Fast forward to my being sent to the psych unit, about which I no longer had any choice, being labelled violent now and OOC as well as mute and schizophrenic (I hate that word but they used it). When the doctor who admitted me, Dr. Michael Balkunas, came to see me the next day, I was still mute. He asked me how I was and I gestured my need for a writing implement to answer his questions. He coldly told me that he would not speak with me if I would not talk out loud. Then he got up and walked out the door, with nothing more to say. I was by then so upset and outraged that I got up off the bed, which was the only furniture in the room, and slammed the door after him. I meant only to make a noise to express my frustration, but unfortunately it caught him in the shoulder. This was not intentional, not that I recall, though I confess I was so enraged by his dismissal of me, especially after the violence inflicted on me not once but twice the night before in the ER on his orders, that it is possible I wanted the door to make contact with him. What I know is that I most certainly did not intend to injure him. I only wanted him to know, before he walked away from me, that I was angry and “speaking” to him the only way I could. Dr. Balkunas’s reaction was itself swift and violent in the extreme, and extremely personal. Enraged, his face beet-red, he bellowed at the nurses to order guards to force me into “Seclusion! Seclusion! Restraints! Restraints!”
Before I could do anything or even assent to walk there, I was bodily dragged down the hall by my injured shoulder, to one of the most horrifying seclusion suites I have ever seen. A set of two cells, each lockable from the outside, completely barren and cold except for a concrete bed set into the concrete wall, with a plastic mattress on it. Nothing else. No commode, no bed pan, nothing but two obvious cameras in the ceiling, but no obvious way for me to communicate with anyone. They locked me in, locked the second door a room away, so I was thoroughly alone and soundproofed from the rest of the unit, and walked away. I panicked immediately, and urinated on the floor in my panic. I took off my clothes. I screamed — wanting someone to talk to me, I wanted warm dry clothing to wear, but there was no response. I screamed and screamed. Nothing. Not a word. I did not even understand at that time that there was an intercom they could hear me through. I thought I was completely alone and abandoned, but for the eye of the camera. So I did what I had to. I KNEW what would happen, I knew this because it was SOP. But I was freezing in there, with the A/C on full bore and at 110 pounds and a history of frost bite I cannot tolerate being cold. I also had NO inkling as to how long they would keep me there, one hour or sixteen. All I knew was that I could not tolerate the isolation, one, and I would not survive the freezing temperature, two.
So I took the urine-wet johnnie I had taken off and I rolled it into a rope and tied it around my neck. I pulled on it as if to strangle myself. It was useless of course, because I couldn’t keep pulling it without letting go and then I would breathe. And I didn’t want to die, I just wanted it to LOOK as if I were strangling myself so someone would come in and I could explain that I was COLD! Well, finally the intercom crackled to life and someone said, “Pamela, take that away from your neck now.” I gestured something that clearly indicated, “I’m freezing cold!” The voice spoke again, “If you don’t remove that from your neck, we will restrain you.” I answered silently but in clear gestures, “I need something warm to wear!” Well, this was a battle I was destined to lose, of course. And eventually but not so quickly as to indicate that they were seriously concerned about my safety, guards and nurses entered the room, along with a gurney, and they did as they had threatened, injuring me in the process. They grabbed me and hoisted me onto the gurney and locked me into leather restraint cuffs, in a painful and illegal spread-eagle position, despite my groans of pain and protest, then they refused even to cover me with a blanket. Someone threw a small towel over my lower torso and that was all. They they positioned an aide at the door and trooped out. I screamed my lungs out, and gestured my desperate need for water and warmth, but the aide simply ignored me, saying she wasn’t permitted to talk to me, and couldn’t get me what I needed. That was how violent I was. And that is how the most violent patients are treated and why they MUST be restrained, for their own safety and the safety of others…Right? NOT! ALL the other times I was secluded it was because i was disturbing the peace of the unit. I was loud and complaining, or simply “agitated” because i walked the halls too much.
That was it. That is the rule not the exception, and if you read my posts about my incarceration at the Hartford Hospital Institute of Living in the winter of 2013 you will get a similar picture. I am not the 300 pound crazed man on PCP wielding a weapon, no, I am a small, elderly woman who is non-compliant with the unit milieu and wants only to be warm…that is about it. But each and every hospital claimed that I had to be restrained, that they had NO alternative, that I was so violent that they had no choice, even though it often took only one or two people to do so, because I didn’t resist or say a word, just lay there while they pinioned me to the bed. Now you tell me that restraints and seclusion are necessary ‘modalities of treatment” that cannot be done away with because they might be needed in an emergency. Emergency schmergency. I am that emergency and they were and are NEVER needed, EVER.

TO FORGIVE IS…
To begin and there is so much to forgive
for one, your parents, one and two,
out of whose dim haphazard coupling
you sprang forth roaring, indignantly alive.
For this, whatever else followed,
innocent and guilty, forgive them.
If it is day, forgive the sun its white radiance
blinding the eye;
forgive also the moon for dragging the tides,
for her secrets, her half heart of darkness;
whatever the season, forgive it its various assaults
— floods, gales, storms of ice —
and forgive its changing; for its vanishing act,
stealing what you love and what you hate,
indifferent, forgive time;
and likewise forgive its fickle consort, memory
which fades the photographs of all you can’t remember;
forgive forgetting, which is chaste and kinder
than you know; forgive your age and the age you were when happiness was afire in your blood
and joy sang hymns in the trees;
forgive, too, those trees, which have died;
and forgive death for taking them, inexorable as God; then forgive God His terrible grandeur, His unspeakable Name
forgive, too, the poor devil for a celestial falll no worse than your own.
When you have forgiven whatever is of earth, of sky, of water, whatever is named, whatever remains nameless
forgive, finally, your own sorry self, clothed in temporary flesh,
the breath and blood of you already dying.
Dying, forgiven, now you begin.
by Pamela Spiro Wagner in “We Mad Climb Shaky Ladders” (Cavakerry Press 2009) also featured in “Divided Minds: twin sisters and their Journey through schizophrenia.”

When I was at New Britain General Hospital in the spring of 2014, the security guards stripped me naked and left me in the freezing and barren seclusion room…This is a depiction of a younger woman largely because no one gives a damn about what happens to a 61 year old woman anywhere..but the seclusion room is pretty danged accurate.




ON NOT SPEAKING
When I went temporarily mute at age sixty,
it sparked no visual wonders.
After decades schooled by dictionaries,
vocabulary categorized the world:
“precipice,” “acrid,” “blanch;”
words even defined my senses.
But one can fall into
speechlessness for reasons
beyond pathology
though these may not seem reasonable
to people who believe that only talking things out
or about them makes sense.
Speaking or not, I knew
when silence was less insane
than trying to be heard
by those who would rather hurt me
than pay attention.
But if, as they say, silence is so eloquent,
why couldn’t anyone hear
what I so desperately didn’t say?
I want to reblog this brilliant post by Anne C. Woodlen and then i will add my own editorial comments if i can in a later post or edit. In the meantime, i think it speaks for itself and says just about what i would want to tell a lot of young people newly diagnosed with bpd or did or add or even bipolar disorder and getting on disability, preparing for a life “in the system” – it sucks and it isn’t worth it unless you are floridly psychotic. And even then, don’t believe what they tell you about antipsychotic drugs. There ain’t no such medication, only sedatives that may or may not quiet things down temporarily. The only way out is through, if you can do it with a wise and caring guide and community. Don’t get stuck as i am, on multiple antipsychotic drugs, addicted to them so that getting off them only means you get more psychotic than ever. Psychosis need not be a lifelong problem, but it certainly will be if you keep taking high doses of the drugs and never explore other options.
Behind the Locked Doors of Inpatient Psychiatry
Hello,
My name is Dustin and I live in Michigan. When I was seventeen years old my mother put me in a psychiatric hospital called Forest View. The abuse I felt violated me to the core! I felt like I was being raped having to submit to all the rules, the bullying and the emotional abuse. To have your dignity removed when you are an innocent patient and just want genuine, kind, gentle care, and get unprofessional jerks who you can tell are fake and just care about getting paid is a horrible experience. If anything it only caused me more traumas with the trauma that I already had. I am now twenty-two years old and live on disability while also living my life as a hermit because now I am afraid of people due to the awful treatment I endured. I was diagnosed with Borderline Personality Disorder by a REAL…
View original post 856 more words






As my time here comes to an end, I will miss it and my neighbors terribly., I don’t know what I will do without them, and Lydia my wonderful companion. Returning to Connecticut with its horrible hospitals and indifferent treatment just feels like a disaster waiting to happen. I want to move to Vermont but I don’t know how I can make that happen. I have felt amongst friends everywhere here, but isolated completely for years in CT, despite my lovely dear friends there, I wish I could bring them all up to VT with me!
This video is pretty sickening and difficult to watch. However it is brief and necessary, if you care about what the police are doing tp everyday citizens in this country… (Need I mention that Eric happens to be African American, which I believe was significant in his treatment, just as a mental illness would have been or other supposedly extraneous factors…



Pamela Spiro Wagner’s apartment is full of art she’s made while in psychiatric care. One piece dominates the room. It looks like a painting at first. It shows a threadbare seclusion room and a restraining bed.
“That’s made of Vogue magazines. If you look at it, you’ll see there’s a little label of Prada leather on the leather restraints, which was done on purpose,” Wagner said. She made it while alone in a hospital seclusion room. The magazines were the only art supplies she had.
Wagner has schizophrenia. She’s been in and out of Connecticut hospitals for decades, and she knows what it’s like to be restrained. “They use leather, or rubber, or plastic, or whatever restraints that they wrap around your wrists, usually tight because they don’t want you to get out. They pull them as tight as possible to the sides of the bed,” she said.
Wagner was put in four-point restraints. That means each limb is bolted to the bed, and she said she’s stayed there for nearly a day at a time. “I would just scream from the base of my lungs,” she said, “like the screams that if you had any heart, your heart would break if you heard me scream.”
“Restraint is Pretty Traumatic”
Patricia Rehmer, Commissioner of the Connecticut Department of Mental Health and Addiction Services, said the department has cut down on restraint since receiving a federal grant in 2008. “We know,” she said. “The literature is clear; the clients are clear. Seclusion and restraint is usually a pretty traumatic event. If we had our way, there would be no seclusion and restraint. We’d love to get to zero, but that’s not always possible.”
The Department of Mental Health and Addiction Services oversees state hospitals in Bridgeport, New Haven, Hartford, and Middletown. Rehmer said that because patients stay longer at state hospitals, doctors and nurses have more time to work with them on ways to avoid restraint. “Frankly, there are differences between our hospitals, our hospital beds, and general hospital beds, for example,” she said.
Read C-HIT Report: State Restrains Psychiatric Patients at High Rate
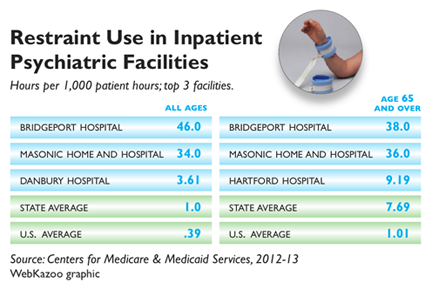
Restraining or secluding patients used to be commonplace in psychiatric facilities, but ten years after a series of deaths nationwide, there’s been a push to lessen the time patients spend restrained. Federal data released earlier this month showed that Connecticut’s rates of restraint are still high compared to most of the country – more than double the national average. The state ranks eleventh nationwide, and third for use of restraints among the elderly.
Connecticut Institutions Adapt
Bridgeport Hospital topped the list statewide. The hospital has a large geriatric unit, and the numbers were high for elderly patients.
“We realized about a year and a half ago that we were really having a problem,” said Ryan O’Connell, Bridgeport Hospital’s vice president of performance and risk management. He pointed out that the numbers only go up to the middle of 2013, and said that the hospital started changing its practices since then. “It was much more common for us to go to some type of restraint,” he said.
O’Connell said the image of the barren room and four leather straps is all wrong at Bridgeport. They’re mostly trying to keep patients with dementia from wandering off and into danger. “I think it’s really important,” he said, “that nobody thinks that we were tying people down [by their] hands and feet.”
Bridgeport is moving toward something called comfort rooms, with colorful wallpaper, toys, games, or comfortable furniture. They’re becoming common alternatives in a lot of institutions, like Connecticut Valley Hospital in Middletown — a state hospital that cut back on using restraints by about 88 percent in the past decade.
In 2002, a patient died after being restrained at CVH. The hospital conducted investigations after the death, but Director Charles Dike said they’d already decided to make a change before it happened. “Our target is to make sure we use it as sparingly as possible, only when it is absolutely necessary, and that we discontinue it as quickly as possible,” he said.
CVH started using comfort rooms years ago. Dike said that instead of putting a patient in restraints, they try to encourage a patient to spend a little time alone doing something relaxing. He said, “If somebody says to me, when I’m not doing so well, I like to go into my room and play music, and that helps me calm down…” He said that nurses will remember, and bring it up if the patient starts to lose control.
Dike doesn’t expect to stop using restraints. He said there will always be outliers — patients who come straight from emergency rooms and prisons.
Ellen Blair is the nurse director at Hartford’s Institute of Living, which is part of the Hartford Hospital system. Figures for 2013 show Hartford Hospital restrains patients at a little over the state average, but she said they’ve cut back since then thanks to new training programs and more comfort rooms.
Blair said that when a patient does go into restraints, they’re looked after. “I personally go and make sure I know that patient,” she said. “We all talk about it at least every couple of hours, because we don’t want to keep it going any longer than we have to.” She said patients aren’t left alone, and that restraint is only used as a last resort when patients are dangerous to themselves or others.
“Every day,” Blair said, “we come here thinking, okay, we’re going to have a good day. We’re going to prevent people from getting agitated and having to go to that level.” Restraint, however, remains a last resort these hospitals said they don’t plan to take off the table entirely.

Lots to say about the situation I am in up here in Vermont, where my assistant, the person hired to help me and make sure things go okay turned out to be a common criminal. But I am too tired and worn out by having to deal with the mess left in her wake to write about it. Suffice it to say that she stole my debit/credit card number and racked up multiple charges, was apparently drinking even in the mornings without my knowing it, and driving me at the same time. She had a hand bag full of narcotics not all of them prescribed to her, but even if they had been, what was she doing, taking narcotics and drinking and driving?!
Things were even worse than that, but as I said, I am exhausted and cannot go into it all now. Needless to say, she has been fired and is gone, is out of here…But she has left a mess and misery in her wake all around. What a mess maker! And I think she was the one who was stealing from me all the while last winter when I had people staying with me to prevent a hospitalization…Why did I once trust her implicitly? Where do I find these people and WHY do I trust them at all?
I should have known something was wrong when I saw her handbag full of Percocet and Xanax and VIcodin and fentanyl patches etc. It was ridiculous…and then to have her buy a case of beer? But I thought “well, a beer once in a while is harmless.”…I didn’t know she was drinking at breakfast and also while driving…I am such a dimwit!

LONDON ― A novel treatment may help patients with schizophrenia confront and even silence the internal persecutory voices they hear, new research suggests.
Avatar therapy allows patients to choose a digital face (or “avatar”) that best resembles what they picture their phantom voice to look like. Then, after discussing ahead of time the things the voice often says to the patient, a therapist sits in a separate room and “talks” through the animated avatar shown on a computer monitor in a disguised and filtered voice as it interacts with the patient.
In addition, the therapist can also talk by microphone in a normal voice to coach the patient throughout each session.
In a pilot study of 26 patients with treatment-resistant psychosis who reported auditory hallucinations, those who received 6 half-hour sessions of avatar therapy reported a significant reduction in the frequency and volume of the internal voices ― and 3 reported that the voices had disappeared altogether.
“Opening up a dialogue between a patient and the voice they’ve been hearing is powerful. This is a way to talk to it instead of only hearing 1-way conversations,” lead author and creator of the therapy program Julian Leff, MD, FRCPsych, emeritus professor at the Institute of Psychiatry in London, told meeting attendees.
 |
|
Dr. Julian Leff
|
“As the therapist, I’m sharing the patient’s experience and can actually hear what the patient hears. But it’s important to remind them that this is something that they created and that they are in a safe space,” Dr. Leff told Medscape Medical Newsafter his presentation.
Two presentations were given here at the International Congress of the Royal College of Psychiatrists (RCPsych) 2014 the day after the study results were released in the print edition of Psychosis.
Regaining Control
According to the investigators, 1 in 4 people who hear phantom voices fail to respond to antipsychotic medication.
Dr. Leff explained that this program started a little more than 3 years ago, after he had retired “and could start thinking clearly again.” He had been interested in the phenomenon of phantom voices for more than 40 years.
“Our mind craves meaningful input. That’s its nourishment. And if it’s deprived of nourishment, it pushes out something into the outside world,” he said. “The aim of our therapy is to give the patient’s ego back its mastery over lost provinces of his mental life.”
The researchers used the “off-shelf programs” Facegen for the creation of the avatar faces and Annosoft LIP-SYNC for animating the lips and mouth. They also used a novel real-time voice-morphing program for the voice matching and to let the voice of a therapist to be changed.
In fact, Dr. Leff reported that one option the program provided changed his voice into that of a woman.
After a patient chose a face/avatar from among several options, the investigators could change that face. For example, 1 patient spoke of hearing an angel talk to him but also talked about wanting to live in a world of angels. So the researchers made the avatar very stern and grim so that the patient would be more willing to confront it.
Another patient chose a “red devil” avatar and a low, booming voice to represent the aggressiveness that he had been hearing for 16 years.
For the study, 26 participants between the ages of 14 and 74 years (mean age, 37.7 years; 63% men) were selected and randomly assigned to receive either avatar therapy or treatment as usual with antipsychotic medication.
The length of time for hearing voices ranged from 3.5 years to more than 30 years, and all of the patients had very low self-esteem. Those who heard more than 1 voice were told to choose the one that was most dominant.
Pocket Therapist
|
|
|
Dr. Julian Leff shows examples of faces used in avatar therapy at RCPsych 2014.
|
During the sessions, the therapist sat in a separate room and played dual roles. He coached the participants on how to confront and talk with the avatars in his own voice, and he also voiced the avatars. All of the sessions were recorded and given to the participants on an MP3 recorder to play back if needed, to remind the patients how to confront and talk to the auditory hallucination if it reappeared.
“We told them: It’s like having a therapist in your pocket. Use it,” said Dr. Leff.
All of the avatars started out appearing very stern; they talked loudly and said horrible things to match what the patients had been reportedly experiencing. But after patients learned to talk back to the faces in more confident tones, the avatars began to “soften up” and discuss issues rationally and even offer advice.
Most of the participants who received avatar therapy went on after the study to be able to start new jobs. In addition, most reported that the voices went down to whispers, and 3 patients reported that the voices stopped completely.
The patient who confronted the red devil avatar reported that the voice had disappeared after 2 sessions. At the 3-month follow-up, he reported that the voice had returned, although at night only; he was told to go to bed earlier (to fight possible fatigue) and to use the MP3 player immediately beforehand. On all subsequent follow-ups, he reported that the voice was completely gone, and he has since gone on to work abroad.
Another patient who reported past experiences of abuse asked that his avatar be created wearing sunglasses because he could not bear to look at its eyes. During his sessions, Dr. Leff told him through the avatar that what had happened to the patient was not his fault. And at the end of 5 sessions, the phantom voice disappeared altogether.
Although 1 female patient reported that her phantom voice had not gone away, it had gotten much quieter. “When we asked her why, she said, ‘The voice now knows that if it talks to me, I’ll talk back,’ ” said Dr. Leff.
“These people are giving a face to an incredibly destructive force in their mind. Giving them control to create the avatar lets them control the situation and even make friends with it,” he added.
“The moment that a patient says something and the avatar responds differently than before, everything changes.”
In addition, there was a significant reduction in depression scores on the Calgary Depression Scale for Schizophrenia and in suicidal ideation for the avatar participants at the 3-month follow-up assessment.
A bigger study with a proposed sample size of 140 is currently under way and is “about a quarter of the way complete,” Dr. Leff reports. Of these patients, 70 will receive avatar therapy, and 70 will receive supportive counseling.
“In order for others to master this therapy, it is necessary to construct a treatment manual and this has now been completed, in preparation for the replication study,” write the investigators.
“One of its main aims is to determine whether clinicians working in a standard setting can be trained to achieve results comparable to those that emerged from the pilot study,” they add.
“Fascinating” New Therapy
“I think this is really exciting. It’s a fascinating, new form of therapy,” session moderator Sridevi Kalidindi, FRCPsych, consultant psychiatrist and clinical lead in rehabilitation at South London and Maudsley NHS Foundation Trust in the United Kingdom, told Medscape Medical News.
 |
|
Dr. Sridevi Kalidindi
|
“I think it is a novel way of approaching these very challenging symptoms that people have. From the early results that have been presented, it provides hope for people that they may actually be able to improve from all of these symptoms. And we may be able to reduce their distress in quite a different way from anything we’ve ever done before.”
Dr. Kalidindi, who is also chair of the Rehabilitation Faculty for the Royal College of Psychiatrists, was not involved with this research.
She added that she will be watching this ongoing program “with great interest.”
“I was very enthused to learn that more research is going on with this particularly complex group,” said Dr. Kalidindi.
“This could be something for people who have perhaps not benefitted from other types of intervention. Overall, it’s fantastic.”
International Congress of the Royal College of Psychiatrists (RCPsych) 2014. Presented in 2 oral sessions on June 26, 2014.
Psychosis. 2014;6:166-176. Full text
Original Article From MEDSCAPE:

Not sure what to make of this painting, but I enjoyed doing it…What do you think? It is 8 by 12 inches, approximately, in gouache on Ampersand board (essentially gessoed masonite).

These huge 3-inch to 5-inch moths are not endangered but you have to find them after midnight in or near the woods, before the birds eat their bodies in the early hours of the morning. If you can preserve them for another nighttime, you may rescue these mouthless, non-eating creatures for their prime task, which is mating. The males live to breed and will mate and mate again, but the female, once she has mated, will go on to lay eggs anywhere she can until she is eaten or simply dies at the end of summer. When you rescue a single male you can almost hear the noise made by the rasping bristling antennae as it searches for the scent of the female, which is the one that gives off pheromones of desire for the male, then waits for a mate to come calling on her.
Steffie rescued these two from her house’s outer walls. And I photographed them inside the bucket where they were safe, we thought, until one got scared or attracted by the scent of a female and flew off (despite it being the middle of the morning when they are almost always inert.) The other survived over the day and was revived the next night in order to go out and to find a mate.

I was told by Marc and Steffie, with whom I am staying, that the sea or water represents the unconscious in some schools of thought. Which certainly makes sense to me, given how I titled this very small painting. I painted the blackbird in the stormy sky last, and can see that as a sort of link between the world of life and death, like Van Gogh’s black birds in the fields in his final paintings. But also the notion that the rocking chair can calm the stormy waters, indeed the raging tidal wave of waters outside the room, so that they become only waves but not so disturbing inside, seems to me significant. So, two questions for the pychologically or analytically minded: Why is the room red, one, and why is the chair empty? (I am serious. If you have any ideas or suggestions, I would be curious and eager for your and any interpretation. No need, just interested.)
In any event, in my sleeplessness last niight, I panicked, because I “knew” I couldn’t paint. so I put aside my decent ampersand boards, coated this bit of matboard with black to “ruin” it first, then just went to town, painting the first thing that came to mind. The chair was in the living room, but the rest was purely my imagination. If I knew what I was doing, I confess I would have painted the chair last, ON TOP of the background, but of course, I had no idea what I was doing, so I had to paint it and repaint it as ideas came to me…Hence the messiness! Hope you enjoy!
Ceterum censeo MAGA esse delendam.
The opinions expressed are those of the author. You go get your own opinions.
Kate Greenough's daily drawings
Réussissez toutes vos certifications de langues
Not your third grade paper mache
Portrait Art and Paintings by Jon Amdall
Books, papers and blogs by Joanna Moncrieff
"While I breathe, I hope"
My Life After Narcissistic Abuse
An intellectual, emotional and spiritual spittoon.
The latest news on WordPress.com and the WordPress community.
Everything Matters
Ceterum censeo MAGA esse delendam.
The opinions expressed are those of the author. You go get your own opinions.
Kate Greenough's daily drawings
Réussissez toutes vos certifications de langues
Not your third grade paper mache
Portrait Art and Paintings by Jon Amdall
Books, papers and blogs by Joanna Moncrieff
"While I breathe, I hope"
My Life After Narcissistic Abuse
An intellectual, emotional and spiritual spittoon.
The latest news on WordPress.com and the WordPress community.
Everything Matters

