(I myself think she’s full of sh— and worse, but if anyone wants to discuss this with me, please read below, or find the podcast and listen to it, then come back and tell me what you think.)
Look for First Person, a New York Times podcast, and the February 16, 2023 broadcast, as I don’t know how to put it up here. The transcript is below, but it’s important as well to hear it, to hear the mothers voice etc.
You won’t be able to listen here, as this photo below is just a screenshot, but it shows you what to look for in your podcast offerings.
TRANSCRIPT
He Was ‘Losing His Mind Slowly, and I Watched It’
How do you help someone who doesn’t believe he is mentally ill?
Thursday, February 16th, 2023
This transcript was created using speech recognition software. While it has been reviewed by human transcribers, it may contain errors. Please review the episode audio before quoting from this transcript and emailtranscripts@nytimes.comwith any questions.
Lulu Garcia-Navarro
From New York Times Opinion, I’m Lulu Garcia-Navarro. And this is “First Person.” Late last year, New York City Mayor Eric Adams made headlines.
Archived Recording (Eric Adams)
I want to talk to you about a crisis. We see all around us people with severe and untreated mental illness who live out in the open on the streets —
Lulu Garcia-Navarro
He directed emergency workers to transport more people to the hospital for psychiatric evaluations, whether they wanted to go or not.
Archived Recording (Eric Adams)
These New Yorkers and hundreds of others like them are in urgent need of treatment and often refuse it when offered. The very nature of their illnesses keeps them from realizing they need intervention and support.
Lulu Garcia-Navarro
And on the other side of the country, this year California is rolling out a new court system to monitor people with serious mental illness and potentially compel them into treatment. These programs are extremely controversial. Opponents like disability rights groups say that forced treatment criminalizes mental illness, doesn’t work, and also doesn’t address the real issue — a lack of care and housing for the people who do want it.
And most importantly, they argue that it’s a violation of a mentally ill person’s civil rights. For caregivers like Kimberly, a mom in California, this is not an abstract debate. Her 22-year-old son has been cycling in and out of psychosis since he was a teenager. And as she’s watched him get sicker over the years, she’s wondered if the only way she’s going to save his life is by being in control of it.
And a note — because of the sensitive nature of this story, we’ll only be using Kimberly’s first name, and we won’t be naming her son at all to protect his privacy and medical history. Today on “First Person,” the case for involuntary treatment.
[MUSIC PLAYING]
Kimberly, can you tell me about your son? What was your relationship like when he was little?
Kimberly
My son and I were really close. It was just him and I for quite some time. And he was, I would say, a very attached child. So we did everything together. He didn’t like to be without his mom — very kind, very loving, very enthusiastic. I was his constant play partner because he didn’t have any siblings. And so we just — we did everything together. And I tried to give him the childhood that I never had.
Lulu Garcia-Navarro
How old were you when you had him?
Kimberly
I was 21. I got pregnant by accident. And growing up, I had a pretty traumatic childhood that was pretty chaotic. And so I didn’t plan on having children. And so I was not prepared at all.
I dropped out of college for a bit to raise him. And I struggled going back to work and going back to school at night and on weekends.
Lulu Garcia-Navarro
A lot of sacrifices, it sounds like.
Kimberly
Yes.
Lulu Garcia-Navarro
Before things got hard, what did a good day for the two of you look like?
Kimberly
We used to go to Disneyland a lot. I would pick him up if — on an early day, I would take Fridays off, and I would take him to Disneyland. And it was just him and I spending time together. He loved being outdoors.
Lulu Garcia-Navarro
When did you get the first sign that something might be wrong?
Kimberly
When he was four years old, he would talk about suicide.
Lulu Garcia-Navarro
At four?
Kimberly
Yes. And he would talk about his body image — how he didn’t like his forehead or he didn’t like how fat he appeared, which he didn’t. He was not at all.
He would get night terrors. So I don’t know if that was maybe a sign of — you know, that he could have been battling with something early on, or if it was just, as a young kid, having night terrors.
Lulu Garcia-Navarro
How did you see him start to change as he went through elementary school?
Kimberly
He would still make friends easily. But he would have periods of some conflicts with his friends. And I would always try to resolve them. I was usually friends with his — the parents of his friends.
And then as he got a little bit older, I noticed that he was having more anxiety, not wanting to go to school, refusing to go to school. He was always a smart kid. I tried to start him reading early and doing exercises with him. So he was always on the, I would say, above — ahead of his class a little bit.
And then his grades just took a sharp decline in sixth grade. He would ditch school. I would drop him off at school, and he would walk back home. And I was getting notices of delinquency in the mail. One of the teachers had reached out to me, and she suggested getting him evaluated and seeing a psychologist, getting him into therapy.
And I did. And then he was diagnosed with ADHD. And he was also diagnosed with depression and anxiety.
Lulu Garcia-Navarro
A lot of teenagers obviously struggle with school, anxiety, depression. When did it become apparent that this was actually something more serious?
Kimberly
It became apparent when he started getting more aggressive towards me, punching holes in walls at, like, 13, 14. He’d break things. And he was always a very loving kid and very kind. And so I knew that this was not his personality.
I didn’t know who — what to do or who to turn to. It becomes almost like that dark secret, the way that you’re made to feel a little bit when I reached out to the school. They made it sound like it was my bad parenting that was causing the issue, that I wasn’t strict enough, that I wasn’t disciplined enough.
And so I would try to discipline more and try to enforce more rules and consequences. And that backfired on me. And it only made him more unheard, misunderstood. And it got to the point where I became afraid of him.
He would throw things at me, throw furniture and things. And I could see in his eyes that he was not — he was not there. And looking back, I think that was — during that time, I think he was really just — really going through the process of losing his mind slowly. And I watched it.
Lulu Garcia-Navarro
I’m thinking it must have been terrifying. I mean, you must have been at a loss.
Kimberly
Absolutely. Yes. I was terrified. I didn’t feel like I could share this with most people. It was something that I felt like I needed to hide. The more that I shared, the more it was shocking to other people. And I felt like an outsider.
Lulu Garcia-Navarro
As Kimberly’s son entered high school, she spent more and more of her time trying to get him the help he needed.
Kimberly
Reading all of these books and trying to find out as much as I could that all said it was better to get a diagnosis early on because early intervention, early treatment was the most indication of success.
Lulu Garcia-Navarro
But getting the right diagnosis wasn’t easy. Throughout his early teens, she was told he had OCD, oppositional defiance disorder, conduct disorder. And then he got a bipolar diagnosis. They tried medications, intensive therapy, inpatient treatment. None of it was working.
Kimberly
He would go missing. The psychiatrist, the treatment team, would need to call missing persons. Police would then go out searching for him and sometimes would find him, sometimes would not. And I would need to go out searching for him.
He started not to trust me. He didn’t understand why he needed to be into these programs. He didn’t believe in their diagnosis that he was mentally ill. He didn’t want to appear different from his peers. And it was such a devastating stigma to him.
He was ridiculed by his friends when he would tell them that he had this diagnosis. And so he would resist any type of treatment.
Lulu Garcia-Navarro
So where did you turn next? Where did doctors say it might be good to send him?
Kimberly
His psychologist and his psychiatrist had recommended what’s called a locked facility, an out-of-state school, which was in Utah, because my son had proved that he could not maintain treatment. He needed that type of facility in order to stabilize.
Lulu Garcia-Navarro
So walk me through the thought process of considering sending him to Utah. What was it like to make that choice?
Kimberly
It was horrible. It was one of the hardest things I’ve ever done.
I did a lot of research on these facilities. And there was a lot of mixed reviews. There’s abuse that could go on at these facilities.
And it was extremely hard, you know, the decision to do this. But it was ultimately something I needed to do because he was more at risk staying here, because he was wandering the streets at night. I couldn’t keep him safe. And so they said for his safety, he needed to be in a facility like this.
Lulu Garcia-Navarro
Did you talk to him about going, Kimberly? I mean, did you explain to him why you needed him to go to that facility?
Kimberly
I tried to as best I could, but his psychiatrist had told me I could not talk to him about it actually happening and when it was going to be, because he would run away. And he had told me as much. And he had done as much previously in other programs.
Lulu Garcia-Navarro
How did you get him there?
Kimberly
They recommended a service that is normally hired for these type of situations, that they come in the middle of the night, around 3:00 AM. And they said that I needed to pack a bag for him. And I could not let him see that. And it was three big huge men that came in the middle of the night and woke him up. And they told him to get out of bed, get dressed. You’re coming with us, and you’re going to school in a different program, and say goodbye to your mom, and —
Lulu Garcia-Navarro
Wow.
Kimberly
He wouldn’t even look at me. He was so upset with me and so hurt. I was heartbroken. I think I cried for many days after that and wouldn’t leave the house. I knew that he was going to perceive it as — that I betrayed him. And he did.
Lulu Garcia-Navarro
The facility Kimberly sent him to in Utah is one of the oldest of its kind in the country. It’s part of the so-called troubled teen industry — for-profit schools that offer the promise of stabilization and rehabilitation in a locked down environment. They flourish in Utah because it’s a parent’s right state, meaning that until a child is 18, their parents have the right to make all medical decisions for them.
That’s not the case in California, where Kimberly lives. Until very recently, these schools were largely unregulated. And there has been documented abuse at many of them. Kimberly’s son was 16 when she sent him to Utah. In the end, he’d be there for about nine months.
Kimberly
His experience there was very traumatic. He saw another kid get stabbed in the eye with a pencil. And when first coming into the program, they put him in a very dark room with just a desk to sit at and very minimal. They call it “destimulation” and what they explained to me as taking away all of your natural comforts and privileges that you may feel entitled to or may feel like you have and kind of breaking them down to the bare minimal necessities for behavior modification.
But he was taking medication regularly. He was able to see a psychiatrist regularly and a nurse. He was given therapy a few times a week and group therapy. He was able to finish school and get caught up.
And I think overall, as far as the treatment for it, I think he improved. And he learned a lot in a forced setting. But he held a lot of animosity and anger towards me for this.
Lulu Garcia-Navarro
It sounds awful. I won’t lie.
Kimberly
Yes. It took a long time to repair our relationship and just made him more distrusting of the medications and of any type of professional help, therapy, psychiatrists — completely resistant to it. And he would not answer questions, would not verbalize information. And so I felt like I had to — I had to be his voice.
Lulu Garcia-Navarro
But because he turned 18 and was now an adult, new medical and legal protections had kicked in. And they limited Kimberly’s involvement in her son’s care, even though she had a front row seat to how rapidly he was declining at home.
Kimberly
He was having suicidal thoughts. And he felt that he was losing his mind. He stopped caring about his safety, cutting himself. He hit his head against the wall. He thought people were staring at him and following him around.
He had mentioned he heard the TV talking to him. And he would just spend months locked away in his bedroom.
Lulu Garcia-Navarro
Then on Christmas Eve, when Kimberly’s son was 20, he had a major psychotic episode. He became convinced that there were intruders in the house hurting his mom. He jumped out of a second floor window to get help and was brought to the hospital, where he was put on a psychiatric hold.
There, he received a diagnosis of schizoaffective disorder for the first time and, with it, a new type of medication.
Kimberly
It was the first time they had put him on a long-acting injection which — of an antipsychotic. And they recommended this because of his history of nonadherence to medication. And he started to improve a little bit.
Our relationship was getting better. He was home all the time. His cognition was coming back. He was able to spend time with me, engage.
But he gained 50 pounds in a matter of weeks on this medication, and he’d becomes swollen. And it made him very self-conscious about his image. He did not want to be associated with schizoaffective disorder.
He started to reject the injections. And by March, he completely refused.
Lulu Garcia-Navarro
And by October, Kimberly had become the focus of his paranoia.
Kimberly
He started collecting knives to defend himself against the people that were out to get him. And I learned that I became one of those people that was out to hurt him. And so one night, he had showed up on my balcony, had come in. And he thought that I had stolen from him, and he had a knife. And he pulled a knife on me.
Lulu Garcia-Navarro
So sorry, Kimberly.
Kimberly
I was trying to de-escalate him, and it wasn’t working. And he had a wild look about him. And no matter what I tried to calm him down, I wasn’t able to. My boyfriend was here at the time, and he was able to get him to put the knife down.
And then he had told me to call the police, and I did.
They said that they would arrest him and take him in, and if I wanted to press charges. And I said, no, absolutely not. He needs help.
Lulu Garcia-Navarro
After the break, Kimberly begins to wonder if the only way to get her son treatment that works is to force it on him.
Kimberly
Every time I tried to get him help, they would ask me if I had a conservatorship. And I said, no, no, what’s that? And they said, well, the only way for you to be involved and for us to legally give you information about what’s going on is if you had a conservatorship.
[MUSIC PLAYING]
Lulu Garcia-Navarro
After Kimberly’s son pulled a knife on her, he was taken to the hospital and put on an involuntary 72-hour hold. But the moment that hold kicked in, the clock was ticking. She needed advice. So she turned to the leader of her support group, part of an organization called NAMI, the National Alliance on Mental Illness.
Kimberly
She went through this. Both of her children, sons, had been through this. And so she was telling me, do not allow him to come home. In order to get him help that he needed, I needed to demand from the hospital — I had to say that he had no place to safely live — basically declare him as homeless so that they would keep him in the hospital a little bit longer than a 72-hour period to get stabilized. Otherwise, they were going to discharge him.
Lulu Garcia-Navarro
What was it like to say that he couldn’t come home?
Kimberly
Oh, it was horrible. It was devastating because I basically had to abandon him. And to him, you know, it’s abandonment. When I put him involuntary into the hospital or when I had sent him to Utah, it’s being abandoned by the one person that loves you the most, who loves you unconditionally.
And so to say that you have no place to go to is devastating. In order to get him help, I have to relinquish him into the hands of other people.
Lulu Garcia-Navarro
Kimberly, you did this because you’d gotten advice that it will force the hospital to provide more care beyond a 72-hour hold. Do they at that point?
Kimberly
No. I found out. They kept him over the 72 hours. I think they kept him for about four or five days. But then they said that they would not keep him and they would release him as homeless.
Lulu Garcia-Navarro
And that’s what they did. After Kimberly’s son was discharged, he bounced in and out of short-term facilities, periodically disappearing and wandering the streets for days at a time. Kimberly was frantic. She knew that it was no longer safe for him to live at home. And as she tried to impress the severity of his situation onto his doctors, she kept running into roadblocks.
Kimberly
They will not let you speak to the doctor. You can only speak to a nurse assistant in the office. And oh, well he needs to opt in, in order for you to talk to the doctor, and if he’s already mistrusting, that I need to call the police to get him help.
And it’s not like they go up to him and ask him, hey, will you sign an authorization for the doctor to speak to your mom? That’s not going to happen. And so —
Lulu Garcia-Navarro
You’re stuck.
Kimberly
I’m stuck — nowhere to go, nowhere to turn to you.
Lulu Garcia-Navarro
So she started looking into something that might give her the power to advocate for her son — what California calls an LPS conservatorship.
Kimberly
An LPS is a Lanterman-Petris-Short conservatorship. And it’s specifically for mental illness. One of the criterias for it is they have to prove grave disability. And the criteria is can’t provide food, clothing, or shelter. And it’s extremely, extremely hard to get.
Lulu Garcia-Navarro
And that’s intentional. The LPS conservatorship system was created in the 1960s in response to the practice of locking people up in mental institutions indefinitely. Back then, the bar to subject someone to involuntary treatment was far too low.
So the LPS Act put strict safeguards in place. For one thing, these conservatorships aren’t permanent. And family members can’t request them. A patient has to be referred by a mental health professional. By the way, this is not the same kind of conservatorship that Britney Spears was under.
If a judge approves the LPS conservatorship, a guardian is appointed. Sometimes that’s a family member, sometimes not. But that person can decide where the conservatee lives, consent to medication on their behalf, make medical decisions, and in some cases force treatment.
Kimberly
I thought it would be able to help my son get treatment. When he went into psychosis, he didn’t think that he had this illness. He had what’s called anosognosia — is what I learned is a lack of insight. They don’t recognize it, because oftentimes, they’re in this period of they’re living in a different world that they see that’s very real to them that’s not actually really what’s going on.
And so I’m learning that this is possibly going to be the only way that I could save his life, to get him treatment, and to be able to bring him home, to stabilize him. This is what he needs in order for him to get help, because he is not going to — he’s going to reject it each time.
Lulu Garcia-Navarro
How did you feel about that idea at the time? You’ve talked about how much forcing him to do things had caused damage to your relationship.
Kimberly
My opinion changed over time. As he was getting sick, and I realized — he was around 15 or 16 when he was telling me about the side effects of his medication and he didn’t want to take it. And I thought, he knows what his body is telling him. He knows what’s best. I’ll let him make those decisions.
But going through over the years and seeing him decline without medication, and seeing how bad it got where I’m fearing for my life and I don’t know when he’s going to decompensate so bad where he might kill me, he might kill everyone in our family, he might kill himself, he might kill some random person on the street, and I’m reading these stories in the news, and I’m looking at these mass — these mass murderings, these mass shootings, and I hear people say — like, sarcastically my neighbors will say, oh, their parents must be so proud of them, you know.
And I think to myself now going through it. And I’m like, no, we’re devastated. We’re trying to get help for your kid growing up over and over and being shut down everywhere you go and every turn you go to.
Lulu Garcia-Navarro
Of course, mentally ill people don’t necessarily commit acts of violence.
Kimberly
Correct, yes. Most people with severe mental illness are not violent. But because of the system that we have, the lack of a behavioral health system that works, our system requires them to be violent, to commit a crime.
This is what I was told by the police. They showed up and they said, well, he’s not harming anybody right now. And he’s not in the process of killing anybody right now. So there’s nothing we can do. And they would take it to that extreme, that they would have to see him. They have to observe it in order for him to be hospitalized, to get the help that he needs, because they can’t be forced.
Lulu Garcia-Navarro
So the only way he gets help is if it’s the worst-case scenario. He’s committing a crime against somebody else or he’s threatening his own life.
Kimberly
Correct.
Lulu Garcia-Navarro
What I’m hearing you say is a big roadblock to him being conserved is this criteria for who counts as sick enough. And I guess I’m wondering in theory, does that high bar make sense to you as a safeguard? Because when we’re talking about a system evaluating so many people, it might not necessarily be a bad thing for the system to be slow and cautious when considering such an extreme option.
Kimberly
It’s a hypocrisy, because the medical research says that the earlier intervention happens and the earlier treatment happens, the more successful. And there’s also — there’s cognitive decline. The longer that someone goes into psychosis, it’s neurodegenerative. And so a lot of them revert backwards.
And I have seen that in my son. He is not the same. And each time, he loses more of his intellect, of his ability to function.
Lulu Garcia-Navarro
You see this cautiousness in this case is harmful in some ways.
Kimberly
Yes, absolutely.
Lulu Garcia-Navarro
Does the conservatorship actually seem like a possibility?
Kimberly
It seems impossible.
Lulu Garcia-Navarro
And why hasn’t someone referred him yet?
Kimberly
[LAUGHS]: That’s a question that I constantly have been asking for the past few years. What I found out was that it comes down to funding.
Lulu Garcia-Navarro
Like so much else in the American health care system, it’s a question of who pays. Psychiatric care beds have been disappearing for years. And it’s really expensive to keep people in the ones that do exist.
When a hospital refers someone for conservatorship, they are legally required to keep them until a judge can rule. That process can take months. And it can disincentivize hospitals from referring people in the first place. But money aside, it’s also an ethical question.
Kimberly, I’m thinking about this impossible situation that these mental health care systems put caregivers like yourself in. Speaking more broadly, though, when I hear the word “conservatorship,” I think of people being thrown into institutions indefinitely.
And the director of the Disability Rights Program at the ACLU has actually said, I believe, that conservatorship is America’s most extreme deprivation of civil rights aside from the death penalty. How does that sit with you, that criticism?
Kimberly
Before all of this, before I was as intimately involved, I used to think people should have the right to be in charge of their body, just like how I feel about abortion is that you should — a woman should have the right to decide what happens to their body. I should have the right to decide what — the medication that I take or the right to die, even.
But learning about this, what I now know as anosognosia, is that he didn’t think that he was ill, and knowing that my son is not in a compensatory state where he knows what is medically necessary for him and that he’s going to die — and so I know that is necessary for him, even if it’s temporary, just to stabilize him, so that he can survive, because I know that he’s not likely to survive without it.
And so it makes me angry because I feel like those that are against the forced treatment or the conservatorship are not intimately involved with what’s going on. They have no clue what it is like as a family member to go through this. It’s painful. It’s traumatic. Your whole life takes another course.
Like, all of the dreams that I had for my son — him being happy and just being able to live a normal life — those go out the window. Dreams for myself, for my own life, go out the window. I can’t take vacation like normal people can. I can’t leave him.
People don’t understand what it takes to take care of someone with this illness — through no fault of their own. They didn’t ask for this, and I certainly didn’t ask for this.
Lulu Garcia-Navarro
This word you’ve used a couple of times, “anosognosia,” it’s kind of a controversial one so I want to pause here. It means that a person with a psychotic disorder doesn’t have insight into their illness. They think that they’re fine, even when they’re very clearly not.
And that part is not contested, but it also has come to mean something specific, which you alluded to, which is that mental illness is a neurological condition observable in the brain. And it’s become part of this argument for making it easier to treat people against their will. I mean, you could see how it’s a framework that could be abused. You don’t have to listen to what someone wants for themselves if you can dismiss their preferences as part of their illness. I mean, how would you respond to that concern?
Kimberly
The way I would have liken it to is if someone is out in public, and they are choking and they need CPR to survive, and — you’re not going to ask for permission if someone is not able to make that decision. You’re going to give them CPR.
And this is the way, the same way, that I look at it. No matter what rock bottom my son is going to hit — and he has hit it — he’s not going to ask for help. He thinks that the government’s trying to control him and his body. Or it could be CIA agents poisoning his food in the middle of the night. I mean, these are the things that he thinks. And so he’s not going to opt in for treatment. Some of the times, he has anosognosia and has no insight. And there are other times where he’ll have a moment of clarity. And that’s when — those moments of clarity, I could tell, because his memory starts to come back. He can have a relationship with me. He can have a conversation, even.
When he’s so psychotic that he can’t even speak, he can’t read, he can’t write, he jumps off of buildings, not thinking that he’s going to get hurt. It’s those kind of things where you know that the person is not competent enough to opt in for treatment when they clearly need it.
Lulu Garcia-Navarro
How do you think about what your son wants? I mean —
Kimberly
I would never force anything on him if he didn’t want it except for when he’s in an acute psychotic moment where it’s clear that he is going to hurt himself or hurt somebody else. When I know that it’s heading that way, even if he wants to try different therapies, if he wants to go off of his medication — and I’m OK with that. But when I see another instance when he starts having severe decline, I’d be able to help him get treatment.
These are always the last resort for parents. When you’re so desperate to get help to save your child’s life, that involuntary treatment is always the last course of action that you take.
Lulu Garcia-Navarro
How is your son today? Where is he?
Kimberly
He is in a residential facility. It’s supposed to be an enhanced one that they can dispense medication. But they have to opt in for it.
Lulu Garcia-Navarro
When’s the next time you’re going to see him?
Kimberly
Today. I just saw him last night, and I’m going to see him today. I try to see him as much as possible.
Lulu Garcia-Navarro
And what is that like? How are you two doing?
Kimberly
Yeah, it’s great right now because he’s been on medication. He was hospitalized in October, and then he came out, and he’s been on medication. And we’ve been having a great time.
I’ve been able to take off of work. I took a family leave of absence, and I’ve seen him almost every day. And I’ve learned to have a lot more empathy. I’ve realized how horrible it is and what it must be like to be him and in his brain and the constant just trauma that he goes through.
We have a really good relationship right now. And I’m scared of losing that because I know he’s decided not to take medication again. I’m seeing him start to change a little bit, become more withdrawn and inside of his head. And I’m scared. I’m scared of that.
And I’m exhausted of this fight. And I’m not looking forward to doing this for the rest of — to continue fighting like this. But I will do it because he’s my son. And I’m going to protect him at all costs when I know that he can’t do it on his own.
Lulu Garcia-Navarro
He’s lucky to have you.
Kimberly
Thank you. I’m lucky to have him. I’m just — if I could take this away from him and take it on myself, I would do it in a heartbeat.
[MUSIC PLAYING]
Lulu Garcia-Navarro
“First Person” is a production of New York Times Opinion. If you want to reach us, you can at firstperson@nytimes.com. And please leave us a review on Apple Podcasts.
This episode was produced by Olivia Natt. It was edited by Anabel Bacon and Kaari Pitkin. Mixing by Carole Sabouraud and Isaac Jones. Original music by Isaac Jones, Sonia Herrero, Pat McCusker and Carole Sabouraud. Fact checking by Mary Marge Locker.
The rest of the “First Person” team includes Stephanie Joyce, Wyatt Orme, Rhiannon Corby, Sofia Alvarez Boyd, Derek Arthur and Jillian Weinberger. Special thanks to Kristina Samulewski, Shannon Busta, Allison Benedikt, Annie-Rose Strasser and Katie Kingsbury.
I used to be “crazy.” Labeled CMI, chronically mentally ill, prone to psychosis, i was a revolving door mental patient, one who spent almost as much time in her adult life in the hospital as out of it. Although I had various diagnoses, the main one was schizophrenia, or the variant of it, schizoaffective disorder that some claim combines features of bipolar disorder and schizophrenia. Over time, as I bounced from hospital to home and back to the hospital the doctors would tack on other labels as well, like PTSD and different personality disorders.
Although I occasionally was admitted “voluntarily,” most of these hospital stays started out involuntary, until nurses, brandishing paper and pen, advised me of my right to sign in as “voluntary.” I would sign, but this did not mean I could leave because not even voluntary patients could leave at will, not in the state where I lived at the time. If you wanted to leave before the doctor thought you should, you had to sign a paper stating this. Then wait to see if the doctor challenged the paper. If she did so within three days, you could be taken to probate court for a judge to hear the case. This was never good. We patients knew the judge virtually always sided with the doctors, since we were by definition “crazy” and could not know what was good for us.
But let me go back to the schizophrenia thing. I heard voices, most of the time. They were usually awful voices, voices that jeered and mocked and threatened me, voices that led me to burn myself dozens of times in an effort to rid myself of them. I heard and saw messages to me in everything, from the television and radio ads to newspaper headlines. I saw tiny scintillating red lights that swarmed about me like a cloud of gnats, and which I called the Red Strychnines. I saw Alan Arkin, the actor, and Senator Joe Lieberman dressed as Nazis supervising a conveyor belt sending bodies to the crematorium, and I heard music, people chanting in low voices, unintelligibly at first but later changing to threats. As is often the case, these voices and visions led me to distorted thinking, and to “paranoia,” based on what I heard and saw.
There were other voices. Brother Luke was the name I gave to the one good guy in the lot. He talked to me about time and space and humanity and love, and I felt safe with him. And there were the voices I called the Little People, to distinguish them from the main voices, the bad ones. The Little People occupied objects I used, like my comb or paint brushes and they would talk to one another but would almost never speak directly to me. I could listen in on their lives and concerns, but mostly could not or did not want to interfere. They kept me company with their constant chatter, but they were never threatening or upsetting to me.
The bad voices did bother me, however, and I would often end up in the hospital because of them. But living in a hospital is as bad as it sounds, with horrible food, and little to do, and really no help at all except the constant pressure to take medication, which could turn to threats if you didn’t comply. Worse, if you got out of line, that is, if you got too loud or angry at being kept there or treated by force, they would do things like have a team of security guards strip you naked and lock you in a freezing seclusion cell alone, or shackle your wrists and ankles to a bed, leaving you like that for hours, even days at a time. Or both at the same time. I know this because everything I write about happened to me and on multiple occasions.
Staff called seclusion and restraints measures of last resort, claimed they were only employed when necessary to maintain a patient in safety, but we patients knew they were used almost always as retribution and for punishment. Even SAMHSA (the Federal agency concerned with such things, the Substance Abuse Mental Health Services Administration) knew that restraints and seclusion were not helpful, and were not used as a last resort at all, as they stated in one of their pamphlets:
“… there is a common misconception that seclusion and restraint are used only when absolutely necessary as crisis response techniques. In fact, seclusion and restraint are most commonly used to address loud, disruptive, noncompliant behavior and generally originate from a power struggle between consumer and staff. The decision to apply seclusion or restraint techniques is often arbitrary, idiosyncratic, and generally avoidable (Haimowitz, Urff, & Huckshorn, 2006; NASMHPD, 2003; SAMHSA, 2003).”
In another publication SAMHSA writes:
“Seclusion and restraint were once perceived as therapeutic practices in the treatment of people with mental and/or substance use disorders. Today, these methods are viewed as traumatizing practices and are only to be used as a last resort when less-restrictive measures have failed and safety is at severe risk.”
And this:
“Restraints can be harmful and often re-traumatizing for people, especially those who have trauma histories. Beyond the physical risks of injury and death, it has been found that people who experience seclusion and restraint remain in care longer and are more likely to be readmitted for care.”
But both seclusion and restraints are still used and increasingly so as staff to patient ratios are decreased in psych hospitals and units, with more patients per staff and many staff members poorly trained, if at all.
I don’t believe mental illness is a real entity any more, I don’t believe in schizophrenia or manic-depression or depression or the notion that anyone’s personality can have a disorder. I don’t believe that psychiatry is a valid science or even an art worthy of the name. And I do not believe that we are right on the verge of finally (for the umpteeth time?) discovering the truth about the origins of “mental illness”. We were told the same thing many times before. For instance when the “miracle of psychosurgery” maimed or killed thousands by “helping” them with ice pick surgery and pre-frontal lobotomies. We were told of the miracles of shock, when a variety of drugs as well as electrical current applied to the brain “helped” thousands more, even when bones were broken and people died. And we are still being fed the lie that neuroleptic drugs like Thorazine and Haldol and the new generation of similar drugs like Zyprexa and Risperdal are in fact “antipsychotic” and are an effective treatment for, well, whatever ails you…*
But it was not true that lobotomies helped anyone, shock treatments, which induce grand mal seizures, are by definition brain damaging, and the drugs rarely help more than they hurt, since it has been shown that long term they create more illness, chronic illness, than they ever alleviated.
We should have known this. Back in the 50s when Thorazine was seriously referred to as a chemical lobotomy (which was seen as desirable) doctors noted that the drug was not in fact a treatment that helped the person who took it, reducing symptoms or restoring health. What they saw was that those given the drug became subdued, even immobilized into the infamous Thorazine shuffle, and more “compliant.” This helped the nurses be nurses, as the formerly disruptive were now bludgeoned by Thorazine into mild, shuffling sufferers. They were no longer mad-men or mad-women, no, they had been disabled by the drug and could now be nursed as true patients, patients who were sick and needed nursing care.
I have been given high doses of Thorazine and know from experience that it is a horrible, deadening drug. I have been forcibly treated with soul-killing Haldol and Mellaril and Stelazine and the others, and when Clozaril came out I was given that (thankfully, because the side effects were horrendous, I developed agranulocytosis, twice, so I was taken off it) and then Risperdal and Zyprexa and again, most of the others that later came onto the market. None of them helped me or reduced the voices or made me happier.
Two things did help. Art, which became my life’s passion, and therapy, therapy not with a psychiatrist or an LCSW working under the auspices of a psychiatrist, clinicians who saw only so-called mental illness, but with a woman who does not even have a license to practice in this country. She never saw schizophrenia or bipolar or personality disorders in me when we talked, she saw me, the me beneath all the labels, and she saw me as good, she saw a good person, not the “Satan’s spawn” that the voices derided. She saw me healthy and thriving, even before I did. She did not want to control me, in fact human freedom was and is her main concern. But she accepted me as I was, and her unconditional acceptance and love (for what else was it?) gave me back a sense of self and the self-esteem to thrive and move forward into my life.
I want to say a word about my falling in love with art. I became an artist very suddenly, overnight, in 2008, and this was a miracle in my life. I did not at the time understand how or why it happened, but I woke up one morning with a voice inside my head (all the others seemed to emanate from outside me) telling me, “You must build a human, you must build a human.” Well, I thought, this voice is not telling me to harm myself, so what’s the problem with obeying it? So I set out to build a human, and did in three months, create a life-size papier mâché woman, seated in a paper mâché chair.
Decorated Betsy
Later this won a prize and was bought by an art collector/friend. But it seemed to unleash something in me that drove me to make art constantly from 2008 onward.
It was only in 2017 and later in 2020, when I managed to get off all my psych drugs, that I realized I had also stopped doing art. Was it possible that the drugs were responsible, then, for the miracle I could no longer live without? I went back on them, and within a week or two I was doing art again.
And a second trial of slowly stopping them, which also resulted in my stopping my practice of daily art, led me to the conclusion that without at least one of these drugs, I could not do art. And art was my raison d’être, something I could not live without.
After some lengthy experimentation, I finally determined that it was a drug called Abilify that had produced the miracle of allowing me to do art. Abilify, which I had started in 2008, and which is technically in the “anti-psychotic” class of drugs, is also used along with antidepressants purportedly to help in depression. Nowhere has anyone ever noted its use in stimulating creativity. But that’s what it does for me, and it does so reliably.
Off Abilify, I do no art. On it, on a “therapeutic dose,” I can access my creativity in a way that I can no longer live without. But it decidedly does not act as an anti-psychotic, or as an anti-depressant, because I’m fine these days, and all my “symptoms” — a term I never use except in quotes — all the voices and visions, the distorted thinking and “paranoia” I used to experience are gone, whether I take the drug or not.
I believe that the extreme mental states called “mental illness” all have their origin in trauma, childhood and otherwise, and often these traumas are re-enacted and reinforced by what is absurdly called “psychiatric care.”
Forced medication and forcible treatment, restraints and seclusion and involuntary commitments, all these are liberally employed, as if shackling a person to a bed or chair for hours at a time, or holding someone down for forced injections, is an act of compassion. Note that these measures are undertaken most often against poor people or minorities, and buttressed by the same lies about “anti-psychotics” and “anti-depressants” that are also foisted on the general public.
If psychiatry was a profession entirely dedicated to the truth about each individual and the truth about trauma, and was not so tied to the mercenary interests of the pharmaceutical companies, maybe today it would be a healing profession and not the corrupt, pseudo-medical cabal it is.
The profession could change, become what it purports to be, but this would necessitate psychiatrists looking honestly at history. Alas, I doubt that those who have arrogated so much power to themselves will ever relinquish it, much less acknowledge with remorse the immense harm psychiatry has inflicted on the world.
————————————————————-
* Dr. Heidi Fowler, a psychiatrist at HealthTap wrote this: “Abilify (aripiprazole): Abilify (aripiprazole) is used to treat Schizophrenia, Bipolar Disorder, as an adjunctive medication for recalcitrant major depression; autism spectrum disorders. Off label uses include: dementia; alcohol abuse/dependence and the following for which there are no trials or minimal efficacy: Generalized anxiety disorder, Social phobia, ADHD, agitation, Eating disorders, insomnia, borderline personality disorder.”
I have been able to speak now for at least a month, but before that there were four months of what I can only call subconsciously self-imposed silence. Not “selective mutism” because I did not speak at all. There does not seem to be any term for this intermittent affliction, when I cannot speak for long periods of time, but as my poem says, “Nothing locks my lips or seals my tongue” — a paraphrase I fear because I do not recall the exact words.
I would write more, but I have no time this morning. I post this small, 3.5″ by 2.5″ drawing because of Sue B’s comment on my most recent post…as it most eloquently I think answers her question. Whatever the reason for my muteness, I do not consciously choose to go silent. It simply happens, with a bang, so to speak.
This muteness can lift, I have found, with music, with singing, and people encouraging me to sing…and then to sing-talk my words, until finally I “forget” and simply end up speaking.
Here is the poem I wrote that expresses some of htis, It can be found in my newest book, LEARNING TO SEE IN THREE DIMENSIONS, available on Amazon and through any bookstore.
PHILOMELA
I haven’t spoken out loud for many weeks,
bullied by “voices” to a frightened into myself silence.
Still, what does “speechless” mean
in these days of text-to-speech software,
with its choice of Vikki or Samantha or Victoria voices,
especially when I’m possessed of a blog and writing fluency
enough to speak my mind to my heart’s content?
Even so, being mute is not a manner of speaking.
Yet I tell you I cantalk. Nothing physical impedes
my tongue, or locks my lips
except my brain’s hallucinated snarls,
Jerry Mahoney and Charlie McCarthy thrown
into surrounding shadows
ordering up this stoppage, blockage, blockade.
Now, like Stevens’ fire-fangled bird at the end of the mind
feathered unlucky, tarred, locked in golden cage
my voice remains only a memento
of everything
I wanted to say, but could not get out,
I couldn’t get it out, I could not get it out…
*In the Greek myth, Philomela is raped and has her tongue cut out by Tereus, the husband of her sister Procne. Rendered mute, Philomela weaves a tapestry detailing the crime to inform her sister, who, enraged, takes revenge on Tereus. At the end of the story, both Procne and Philomela are transformed into birds. In some versions of this story, Philomela turns into a female nightingale, while in others she becomes a swallow. However, neither of these birds can sing.
*Jerry Mahoney and Charlie McCarthy are two famous American ventriloquists’ dummies
Recalling my month-long “treatment” at New Britain Hospital a.k.a Hospital of Central Connecticut on Grand Street, in May 2014, under the supervision of Dr. Michael E. Balkunas
Naked in restraints in New Britain Hospital 2014
Only nine days after that last adders-pit hospital —
You still wear sunshades to protect others from you
though no one out here believes they are in peril.
Nevertheless, the staff there described you
as “assaultive,” dangerous to self and others,
unfit for company or visitors.
Neither accurate nor truthful
they wrote lies for the sake of their convenience.
Now you are a week from making new friends
in far northeastern Vermont,
in a place magically named the Kingdom
and it’s a move your bruised mind
requires, still unable to let go of
the half-nelson grip of hospital guards
bent on eliciting pain, who, when told to strip you
then four-pointed you naked to a mattress,
replaying their favorite rape scene,
yanking each limb apart to expose and humiliate, knowing
that the nurses’ own official policy was hands-off
and would protect their asses.
You want truth, you wish for reconciliation
but how, you wonder, does any Truth or Reconciliation proceed
when so many refuse to acknowledge
that hospital staff broke every rule,
stopping short of murder only
because you submitted nick of time,
your terror strangled in a towel they wound
around your head and face,
before they injected punishment drugs into your buttocks,
Please listen to this. You will find Cortland Pfeffers intro fascinating, and of course pamela as usual has much to say!
Here is a little new art to entice, just a small drawing i did while at fhe hostel in Boston during the Hearing Voices Congress. I hope to post that power point soon.
Just want to keep people aware that these things are absolutely continuing to this day. They have not stopped persecuting psychiatic patients just because YOU dont hear about it. Every single thing in this post has happened to me within the last five years, and is still happening to others. Remember, and dont forget it! Your relatives may not talk about it, but it is happening to someone.
Torture in Connecticut’s Institute of Living psychiatric units in 2013Vermont treats its psychiatric patients like criminals, even in 2016Doctor Threatens Restraints and Shot of Haldol – Painting in acrylics c. 18 by 27 inchesIn restraints, being tortured, at Hospital of Central Connecticut “for disturbing the milieuRestraints torture, permitted by W-1 director at HOCC Michael E. Balkunas MD.
Stripped and locked in seclusion for punishment at CT’s New Britain General HospitalTorture in restraints in Brattleboro Vermont ER in 2016John Dempsey Hospital Psychiatry First Floor, U-Conn Health Center, Farmington, CT-restraints torture!
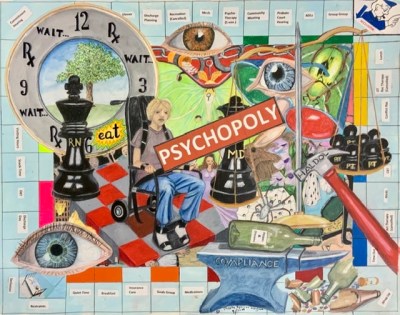
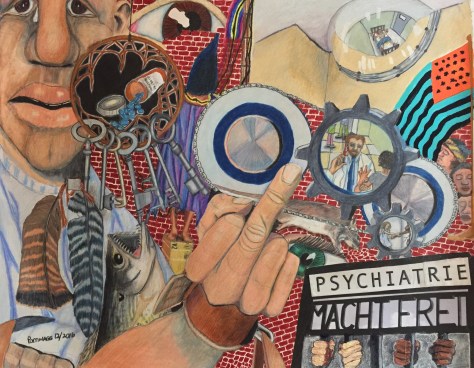
All i can say is everything in this picture was as deliberate as i know how to make it, without planning it at all, and it contains symbolism both public and private. With reference to my signature quotation, (see below) it makes use of what the negative spaces offered me without leaving any in the end.
“There is no negative space, only the shapely void. Hold your hands out, cup the air. To see the emptiness you hold is to know that space loves the world.” P. Wagner
(for those who are not familiar with WWII, over the gates over Auschwitz, the notorious concentration camp where Jews and many other despised groups were taken to be tortured and killed, were emblazoned the words: ARBEIT MACHT FREI, or “work will set you free,” which was of course a lie and a horrible joke, because it was only meant to kill you at what was not a labor camp but just a death camp. )
PSYCHIATRIE MACHT FREI?
Psychiatrie Macht Frei? Mixed media anti-psychiatry picture, 24″by 19″
Psychiatrie Macht Frei? Mixed media anti-psychiatry picture, 24″by 19″
The poem below is the introduction to my third book, and my second book of poems, this time with art, which should be published in the spring of 2017 by Sundog Poetry and Green Writers Press, both Vermont publishers. Wowee!!! I am thrilled. Tamra Higgins of Sundog has generously said that she wants to make sure that I have an art show and reading at the time of the book launching. Moreover I believe that Sydney Lea, Vermont’s wonderful former poet laureate, who had agreed to write the forward for it when it was still going to be published by CKP will still do so for the new publishers. I feel especially blessed!!!
I am very much a novice watercolorist and these are two beginning paintings.
J
TO THE READER
who may be sitting as I am
in a green recliner with a cup of tea
staring out through the porch
to a darkened streetlamp outside the diner,
with a book in her lap, mine, I hope
the only one I feel I should have to mention
if I mention a book in a poem I write;
to the reader, the nitpicker, the one
who may be wondering why
on p. 47 there are two ands, one
right after another, and whose fault that is;
and to the reader, who may be tired
after a long ride home on the bus
after dark and a meal not worth mentioning
who picks up my book but finds his eyes
closing before he has opened the cover,
I say: Forgive me
I am only a writer sitting in a green recliner
with a cup of tea, I can’t explain
those two ands or the mysterious
streetlamp or warm the feet of a tired
reader in his bed. I can only put music on
and tell him stories to make movies
turn in his head, to let him wake
with the sudden understanding that poetry
may be all it takes to make a life—
well, my life at any rate, and maybe his,
and maybe the nitpicker’s and yours, too,
staring through the porch to the streetlamp
where what happens so mysteriously is poetry—
and the whole night is wrapped
in the words spoken by two strangers
meeting there, or not spoken, which is poetry too,
and all of us who listen are waiting
for the music of what is to happen.
Living in a hospital is like living in an Ice Hotel
where all the appointments beneath the furs and fleece
are hard frozen to the floor
Like Ice Hotel staff, the nurses try their best
to be kind, to find compassion for those suffering
here on their sub-zero beds.
But really, they have their warm lives elsewhere.
The psychiatrist knows better. She visits briefly
once a day at the height of the sun, chewing her Vitamin D,
and encourages Hotel visitors to Happy Talk
and Life Skills. If she fails to ease their suffering
in any part, it is because she does not see it, blind
to the fact that the beds are frozen pallets that chill
to the bone. She sees only the furs and warm fleeces.
She cannot fathom why one would not rise and walk
under her cheerful ministrations after a few nights
spent on a banquette of ice. Only the aides
are savvy enough, being low-paid and long-working,
to bring in oil lanterns and hot water bottles.
The patients love them and when finally it comes time
to leave, strange how difficult it is to say good-bye
to even the hardest corner of this place.
_________________________________
luckily i no longer live in a hospital but in a little corner of paradise, in Brattleboro Vermont. And soon I will be writing you about my place. All week i had a headache, which was a beach that was decidely not Miami. But I stopped taking the Abilify on a whim, and wouldn’t you know, immediately the headache ceased. I cannot tell anyone this, because they will become up in arms at my stopping a “necessary medicatoin” but if I do not tell anyone, and things go just fine, won’t that be funny as hell? I think so. And that is precisely what happened when I stopped the Zyprexa, the last time. Everything was fine fine fine,. for six months, and never stopped being fine. I mean I did just as good off it as on it, and we never started it with any good being done, again.
But no negativity from me today. Instead I will leave you with the sunny face painting I did for a member of BRattleboro TIme Trade, in preparation for a papier mache sun we want to work on. Love to all of you!
Sun Face Painting By Pamela Spiro Wagner – plan for papier mache sculpture
Please note that i am reposting this frorm a week ago as it got accidentally deleted, but i cannot repost the comments. Anyone who wishes to recomment is welcome to.
It all started when i bodily “escorted” the nurse,KJ out of my bathroom, where I had situated my mattress, and had her leave my lunch on the table outside. I had been vocalizing loudly and softly virtually only the three words, “oswall wistofi matootam” for days uncontrollably, and over the past hour i had screamed at the top of my lungs from my room, which the nurse had to have heard but made no response. When she simply left my lunch at the table, i felt utterly ignored and abandoned, and in a rage of certainty that she was plotting against me, picked up the cup of coffee and threw it straight at her. With unusual accuracy, it found its target in her center. My next lob hit only the wall.
In certainty of repercussion, i slammed my door and waited. Soon the usual code was called, but instead of burly men bursting in the door, i heard them packing up the sitting area for quite some time, and it knew it took them some several minutes to prepare an injection of my medications. But my terror only increased, so i grabbed a chair to defend my self. Finally they opened the door. KJ in an oh so nice voice said, “pam, i have medication for you.” And they quickly grabbed the chair and four men upended me and laid me on the floor near the bed frame, which was covered in my artwork and books. It took quite some time for the staff to methodically pack up all items they feared, apparently, might go flying at them afterwards ( though if proper protocol had been followed from tHe first, nothing would have).
This proper protocol, by the way, had been developed by another nurse and i after much discussion of my detailed advanced directive and my intense horror of locked seclusion and mechanical restraints, both of which i have experienced in abundance and usually for discipline or convenience, almost never for any truly emergent reason. That said, i believe the first nurse, KJ had lost her temper with me, and decided not to follow this protocol on the unit because she wanted to punish me, as will be demonstrated by what followed.
Having brought the two IM medications with her, which the protocol for agitation we had worked out calls for, she eventually called for the men to deposit me on the bed frame so she could inject them, one in each leg. She did so. Then, instead of having them keep me in a protective hold for as long as i needed to calm myself and potentially fall asleep, which usually took little more than 10-15 minutes, she said, she was having everyone leave and locking me alone in my emptied room. I screamed aloud at this. “I have an advanced directive! You cannot do that!” I pleaded but they forced the door closed against me and locked it.
I screamed to no avail and then started hitting my head in terror against the door in an effort to get them to open it. This worked in a short time, and three aides were sent in. We sat on the bed frame and they actually held my limbs, i thought in such a way as to comfort me. Little did i understand the truth, because even as i very quickly calmed down, soon through the door, the same angry nurse pushed a big prison-issue restraint chair. She yelled at me, “now you are going to have to sit in this!!!
I yelled back, “No!!! No restraints. My advance directive says so!”
I want to interrupt here to quote the government’s own research. SAMHSA’s issue brief #1 March 2010 on promoting alternatives to the use of seclusion and restraints says:
“…the use of seclusion and restraint has often been perceived as therapeutic to consumers. This misconception has been challenged and refuted. Increasing research has identifed the role of trauma in mental and addiction disorders. Research into trauma and trauma-informed care identify common themes about the impact of trauma and how traumatic life experiences can impede an individual’s ability to manage his or her own behaviors or engage in appropriate behaviors in the community.
“Also, there is a common misconception that seclusion and restraint are used only when absolutely necessary as crisis response techniques. In fact, seclusion and restraint are most commonly used to address loud, disruptive, noncompliant behavior and generally originate from a power struggle between consumer and staff. The decision to apply seclusion or restraint techniques is often arbitrary, idiosyncratic, and generally avoidable . Moreover, some studies indicate that seclusion and restraint use leads to an increase in the behaviors staff members are attempting to control or eliminate.”
But they grabbed me and forced me into that chair and despite my struggles and terrified screams of protest they forced nine straps around my body, yes, 9-point restraints because K— J—-, RN, was still angry with me and refused to utilise our calming no-restraints, no seclusion protocol. This protocol had not only helped me but had also since then, so i was told, been used to calm and help other agitated patients without seclusion cells or mechanical restraints after i insisted that the unit staff start doing their “best to avoid restraints” with everyone, not just for me because my A.D insists on it.
Once strapped in to that horrendous chair, i screamed at the nurse, “You are just punishing me!” And calmly, she answered back, “Well, you threw hot coffee at me, what do you expect but punishment!?”
Then she walked out of the room, leaving two aides in the room to tighten the straps so tight that i could not move and felt the circulation in one hand go dead.
In horror, i shrieked for help. I pleaded for anyone to help me, for god’s sake. What the hell were they doing to me?!? Please just help me, someone!!? It upset the other patients to hear this just outside my room. I even begged them to put me in regular 4-point restraints on a bed where at least i could relax and fall asleep. Why hadn’t the nurse not brought me to the seclusion room to begin with, where the walls and door were all were padded if she was not going to follow the protocol?
In the end, it took two hours and two episodes in that terrible chair before they freed me.
That evening, as a response to the trauma, i defecated on the rug in the dining area, and painted with feces on the wall.
Surely this is no way to treat an animal, let alone a troubled psychiatric patient, especially not when there is already a calming,non-violent protocol set up to deal with her when she is agitated?
I say, chairs like this need to be trashed. Once a hospital orders one — and where do they get them? From prison suppliers!) they will use it. They say they use it for emergencies only, but as i have shown, once they have such a chair, it will be used abusively–always, always, always.
The only way to end seclusion and restraints is to stop it now and. For good. The more hospitals dilly-dally saying, soon, we will when we can, they will never stop. There will always been someone to say, no, what about this or that. But abuse is abuse and restraints are abusive by definition. Stop the use of a restraint chair and bed and all use of mechanical restraints by stopping. And then you will find a way to deal with problems arising that work better.
The painting i did below depicts the chair they held me in, minus the waist strap but with the toe restraints.
“There is no negative space, only the shapely void. Hold your hands out, cup the air. To see the emptiness you hold is to know that space loves the world.” P. Wagner
Pamela Spiro Wagner
rutland regional medical center
Rutland vt 05701
These are the latest fractured portraits and artpieces i have done at Rutland Regional Medical Center’s PICU. The portraits are not meant to be recognizably anyone, unless of course, they are. The set of small oil pastels were just experiments. The last picture is a gouache painting, about 22″ by 36″. The others are about half that size and in colored pencil.


















 J
J





 P
P