

https://archive.storycorps.org/search/interviews/?q=Phoebe+Wagner
Category Archives: Mental Health

CRAZY OR NOT, HERE I COME
first published at https://www.blog88.org
by Phoebe Sparrow Wagner
I used to be “crazy.” Labeled CMI, chronically mentally ill, prone to psychosis, i was a revolving door mental patient, one who spent almost as much time in her adult life in the hospital as out of it. Although I had various diagnoses, the main one was schizophrenia, or the variant of it, schizoaffective disorder that some claim combines features of bipolar disorder and schizophrenia. Over time, as I bounced from hospital to home and back to the hospital the doctors would tack on other labels as well, like PTSD and different personality disorders.
Although I occasionally was admitted “voluntarily,” most of these hospital stays started out involuntary, until nurses, brandishing paper and pen, advised me of my right to sign in as “voluntary.” I would sign, but this did not mean I could leave because not even voluntary patients could leave at will, not in the state where I lived at the time. If you wanted to leave before the doctor thought you should, you had to sign a paper stating this. Then wait to see if the doctor challenged the paper. If she did so within three days, you could be taken to probate court for a judge to hear the case. This was never good. We patients knew the judge virtually always sided with the doctors, since we were by definition “crazy” and could not know what was good for us.
But let me go back to the schizophrenia thing. I heard voices, most of the time. They were usually awful voices, voices that jeered and mocked and threatened me, voices that led me to burn myself dozens of times in an effort to rid myself of them. I heard and saw messages to me in everything, from the television and radio ads to newspaper headlines. I saw tiny scintillating red lights that swarmed about me like a cloud of gnats, and which I called the Red Strychnines. I saw Alan Arkin, the actor, and Senator Joe Lieberman dressed as Nazis supervising a conveyor belt sending bodies to the crematorium, and I heard music, people chanting in low voices, unintelligibly at first but later changing to threats. As is often the case, these voices and visions led me to distorted thinking, and to “paranoia,” based on what I heard and saw.
There were other voices. Brother Luke was the name I gave to the one good guy in the lot. He talked to me about time and space and humanity and love, and I felt safe with him. And there were the voices I called the Little People, to distinguish them from the main voices, the bad ones. The Little People occupied objects I used, like my comb or paint brushes and they would talk to one another but would almost never speak directly to me. I could listen in on their lives and concerns, but mostly could not or did not want to interfere. They kept me company with their constant chatter, but they were never threatening or upsetting to me.
The bad voices did bother me, however, and I would often end up in the hospital because of them. But living in a hospital is as bad as it sounds, with horrible food, and little to do, and really no help at all except the constant pressure to take medication, which could turn to threats if you didn’t comply. Worse, if you got out of line, that is, if you got too loud or angry at being kept there or treated by force, they would do things like have a team of security guards strip you naked and lock you in a freezing seclusion cell alone, or shackle your wrists and ankles to a bed, leaving you like that for hours, even days at a time. Or both at the same time. I know this because everything I write about happened to me and on multiple occasions.
Staff called seclusion and restraints measures of last resort, claimed they were only employed when necessary to maintain a patient in safety, but we patients knew they were used almost always as retribution and for punishment. Even SAMHSA (the Federal agency concerned with such things, the Substance Abuse Mental Health Services Administration) knew that restraints and seclusion were not helpful, and were not used as a last resort at all, as they stated in one of their pamphlets:
“… there is a common misconception that seclusion and restraint are used only when absolutely necessary as crisis response techniques. In fact, seclusion and restraint are most commonly used to address loud, disruptive, noncompliant behavior and generally originate from a power struggle between consumer and staff. The decision to apply seclusion or restraint techniques is often arbitrary, idiosyncratic, and generally avoidable (Haimowitz, Urff, & Huckshorn, 2006; NASMHPD, 2003; SAMHSA, 2003).”
In another publication SAMHSA writes:
“Seclusion and restraint were once perceived as therapeutic practices in the treatment of people with mental and/or substance use disorders. Today, these methods are viewed as traumatizing practices and are only to be used as a last resort when less-restrictive measures have failed and safety is at severe risk.”
And this:
“Restraints can be harmful and often re-traumatizing for people, especially those who have trauma histories. Beyond the physical risks of injury and death, it has been found that people who experience seclusion and restraint remain in care longer and are more likely to be readmitted for care.”
But both seclusion and restraints are still used and increasingly so as staff to patient ratios are decreased in psych hospitals and units, with more patients per staff and many staff members poorly trained, if at all.
I don’t believe mental illness is a real entity any more, I don’t believe in schizophrenia or manic-depression or depression or the notion that anyone’s personality can have a disorder. I don’t believe that psychiatry is a valid science or even an art worthy of the name. And I do not believe that we are right on the verge of finally (for the umpteeth time?) discovering the truth about the origins of “mental illness”. We were told the same thing many times before. For instance when the “miracle of psychosurgery” maimed or killed thousands by “helping” them with ice pick surgery and pre-frontal lobotomies. We were told of the miracles of shock, when a variety of drugs as well as electrical current applied to the brain “helped” thousands more, even when bones were broken and people died. And we are still being fed the lie that neuroleptic drugs like Thorazine and Haldol and the new generation of similar drugs like Zyprexa and Risperdal are in fact “antipsychotic” and are an effective treatment for, well, whatever ails you…*
But it was not true that lobotomies helped anyone, shock treatments, which induce grand mal seizures, are by definition brain damaging, and the drugs rarely help more than they hurt, since it has been shown that long term they create more illness, chronic illness, than they ever alleviated.
We should have known this. Back in the 50s when Thorazine was seriously referred to as a chemical lobotomy (which was seen as desirable) doctors noted that the drug was not in fact a treatment that helped the person who took it, reducing symptoms or restoring health. What they saw was that those given the drug became subdued, even immobilized into the infamous Thorazine shuffle, and more “compliant.” This helped the nurses be nurses, as the formerly disruptive were now bludgeoned by Thorazine into mild, shuffling sufferers. They were no longer mad-men or mad-women, no, they had been disabled by the drug and could now be nursed as true patients, patients who were sick and needed nursing care.
I have been given high doses of Thorazine and know from experience that it is a horrible, deadening drug. I have been forcibly treated with soul-killing Haldol and Mellaril and Stelazine and the others, and when Clozaril came out I was given that (thankfully, because the side effects were horrendous, I developed agranulocytosis, twice, so I was taken off it) and then Risperdal and Zyprexa and again, most of the others that later came onto the market. None of them helped me or reduced the voices or made me happier.
Two things did help. Art, which became my life’s passion, and therapy, therapy not with a psychiatrist or an LCSW working under the auspices of a psychiatrist, clinicians who saw only so-called mental illness, but with a woman who does not even have a license to practice in this country. She never saw schizophrenia or bipolar or personality disorders in me when we talked, she saw me, the me beneath all the labels, and she saw me as good, she saw a good person, not the “Satan’s spawn” that the voices derided. She saw me healthy and thriving, even before I did. She did not want to control me, in fact human freedom was and is her main concern. But she accepted me as I was, and her unconditional acceptance and love (for what else was it?) gave me back a sense of self and the self-esteem to thrive and move forward into my life.
I want to say a word about my falling in love with art. I became an artist very suddenly, overnight, in 2008, and this was a miracle in my life. I did not at the time understand how or why it happened, but I woke up one morning with a voice inside my head (all the others seemed to emanate from outside me) telling me, “You must build a human, you must build a human.” Well, I thought, this voice is not telling me to harm myself, so what’s the problem with obeying it? So I set out to build a human, and did in three months, create a life-size papier mâché woman, seated in a paper mâché chair.
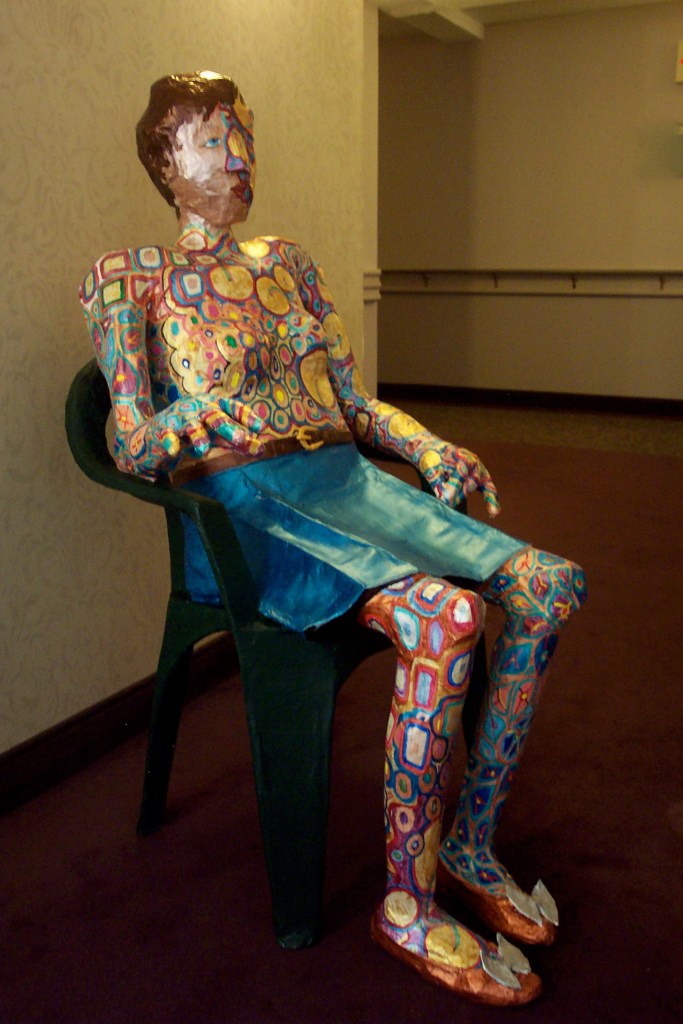
Later this won a prize and was bought by an art collector/friend. But it seemed to unleash something in me that drove me to make art constantly from 2008 onward.
It was only in 2017 and later in 2020, when I managed to get off all my psych drugs, that I realized I had also stopped doing art. Was it possible that the drugs were responsible, then, for the miracle I could no longer live without? I went back on them, and within a week or two I was doing art again.
And a second trial of slowly stopping them, which also resulted in my stopping my practice of daily art, led me to the conclusion that without at least one of these drugs, I could not do art. And art was my raison d’être, something I could not live without.
After some lengthy experimentation, I finally determined that it was a drug called Abilify that had produced the miracle of allowing me to do art. Abilify, which I had started in 2008, and which is technically in the “anti-psychotic” class of drugs, is also used along with antidepressants purportedly to help in depression. Nowhere has anyone ever noted its use in stimulating creativity. But that’s what it does for me, and it does so reliably.
Off Abilify, I do no art. On it, on a “therapeutic dose,” I can access my creativity in a way that I can no longer live without. But it decidedly does not act as an anti-psychotic, or as an anti-depressant, because I’m fine these days, and all my “symptoms” — a term I never use except in quotes — all the voices and visions, the distorted thinking and “paranoia” I used to experience are gone, whether I take the drug or not.
I believe that the extreme mental states called “mental illness” all have their origin in trauma, childhood and otherwise, and often these traumas are re-enacted and reinforced by what is absurdly called “psychiatric care.”
Forced medication and forcible treatment, restraints and seclusion and involuntary commitments, all these are liberally employed, as if shackling a person to a bed or chair for hours at a time, or holding someone down for forced injections, is an act of compassion. Note that these measures are undertaken most often against poor people or minorities, and buttressed by the same lies about “anti-psychotics” and “anti-depressants” that are also foisted on the general public.
If psychiatry was a profession entirely dedicated to the truth about each individual and the truth about trauma, and was not so tied to the mercenary interests of the pharmaceutical companies, maybe today it would be a healing profession and not the corrupt, pseudo-medical cabal it is.
The profession could change, become what it purports to be, but this would necessitate psychiatrists looking honestly at history. Alas, I doubt that those who have arrogated so much power to themselves will ever relinquish it, much less acknowledge with remorse the immense harm psychiatry has inflicted on the world.
————————————————————-
* Dr. Heidi Fowler, a psychiatrist at HealthTap wrote this: “Abilify (aripiprazole): Abilify (aripiprazole) is used to treat Schizophrenia, Bipolar Disorder, as an adjunctive medication for recalcitrant major depression; autism spectrum disorders. Off label uses include: dementia; alcohol abuse/dependence and the following for which there are no trials or minimal efficacy: Generalized anxiety disorder, Social phobia, ADHD, agitation, Eating disorders, insomnia, borderline personality disorder.”
* If you subscribe to Quartz you can read this: https://qz.com/293932/how-this-antipsychotic-became-americas-best-selling-drug/
*Another article on Abilify: https://medtruth.com/drugs/abilify-side-effects/
*Abilify became America’s best-selling drug in 2013-2014, and it was used in myriad ways, not just to “treat” schizophrenia or depression.

MAD FREEDOM NEWSLETTER

This link is to an article by Vicki Warfield and conversation I had with Vicki in December. I hope you read it and enjoy it!
https://us4.campaign-archive.com/?u=4c0f316156312742402b0121c&id=d0fc84805e
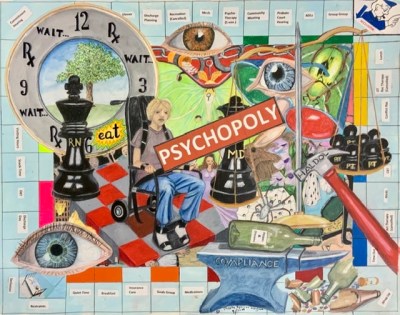
Anti-Psychiatry Art – PSYCHOPOLY

BRATTLEBORO RETREAT — how they torture and abuse patients

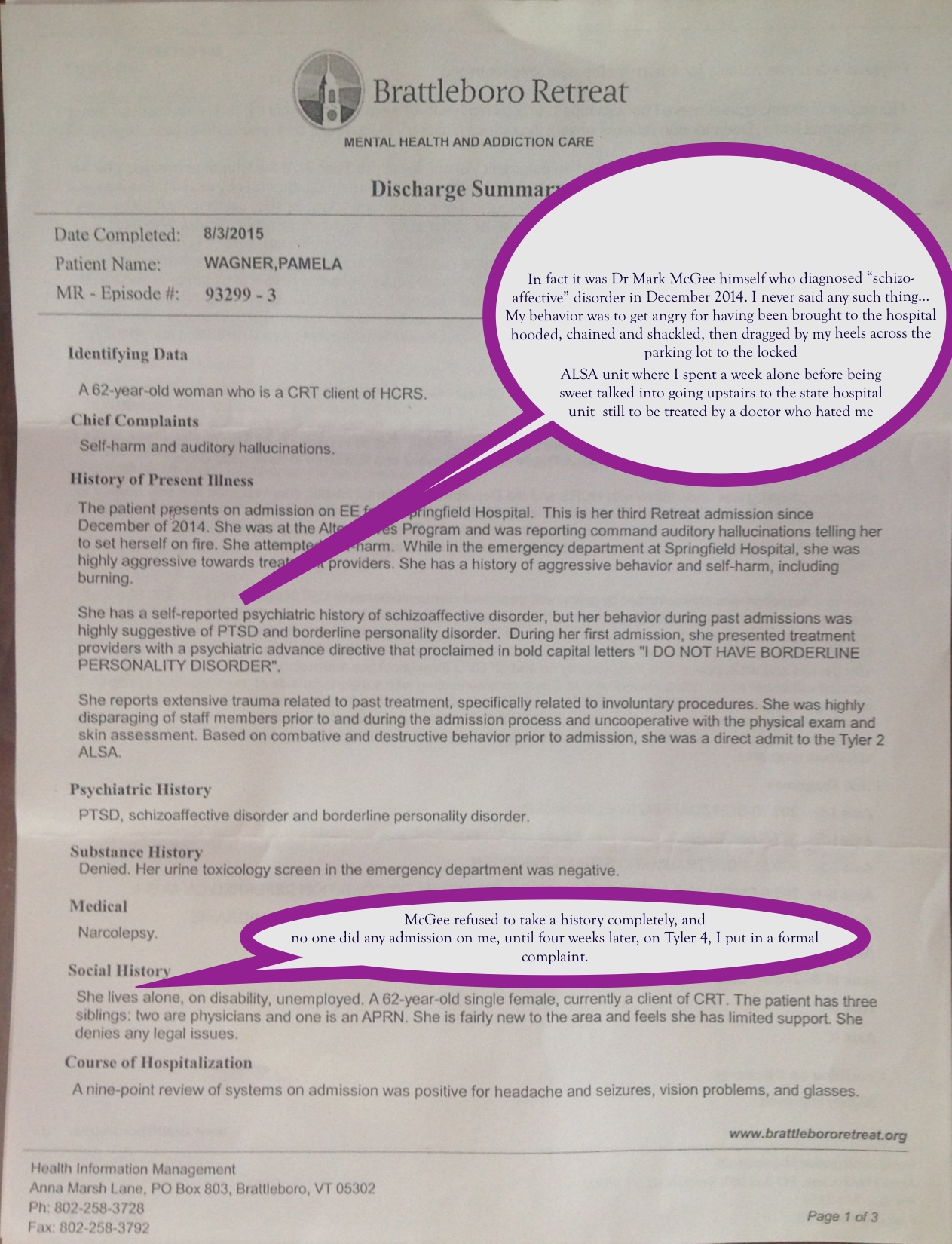
Please read both documents, noting how the first is measured and reasonable written by an impartial social worker, and how the second written By thd doctor who made no bones about how he hated my guts and tries to see BPD in everything, even my socializing and doing art! Jesus flicking christ!

Injuries sustained at VPCH during unlawful restraint
They also broke my glasses.

WHAT REALLY HAPPENED AT VERMONT PSYCHIATRIC CARE HOSPITAL part 1
This was my complaint to the Adult Protective Services, as Licensing and Protection refused to investigate. I AM NAMING NAMES…OF THE GUILTY.
I had been mute for days prior to the date of Nov 18, 2015, when still mutein the early morning, on Unit D at Vermont Psychiatric Care Hospital I started slamming doors because I could not communicate my frustration at not being granted a PRN for Ativan. This was NEVER a danger to self or others. I had done this many times on the unit and was never punished for it, or restrained for it. I also had on file on the unit at that time a signed notarized Advanced Directive on the first 2 pages of which is stated in bold letters the request NOT to use ultimatums or seclusion or restraints because of previous traumatic experiences.
Annette Brennan, the charge nurse, apparently angry with me, came into my room and yelled: “I will not have you slam doors again on my watch!” She then backed me into my tiny bathroom, which I had been using as my bedroom ever since I had been admitted, and grabbed my wrists even though I was mute and unable to object, and when I attempted to biteher fingers to get freeshe called for me to be placed in seclusion.
Once in seclusion, she had staff reenter the seclusion room to have my wristwatch and glasses forcibly taken from me, resulting in injuries to my face and breaking my glasses, even though I was not demonstrating any violence or injurious behaviors, *not* until she called for a team and show of force to gang up on me.
Then she placed me in 5-point restraints only after she had staff reenter the seclusion room and I attempted to leave the seclusion room(if you look carefully at my chart you will see this was the reason for her calling for 5 point restraints and not violence of any sort) despite the Advanced Directive that had been much discussed during my stay in the prior three weeks. This AD states in unequivocal terms that seclusion and use of mechanical restraints has been extremely traumatizing for me and worsens my condition.
Not only that, Nurse Brennan convinced the on call doctor that my lack of speech was volitional and willful and wrote an order which she had Dr. Joseph Lasek sign that I was not to be removed from restraints *until I spoke aloud* NO MATTER HOW COMPLIANT I was, no matter how quietly I lay there. In point of fact they refused to ask me the requisite questions to let me out of restraints even though I lay so still I triggered an assessment every fifteen minutes… This order resulted in severe trauma and several hours of restraints. PLEASE NOTE that no one disputes the fact that I was mute and had been mute for days before this night. This order and Nurse Brennan’s part in what happened was torture. It constituted punishment and unnecessary restraint. None of it was necessary but Ms Brennan was angry with me for an episode of swearing that had occurred several weeks earlier and she lost her temper and her cool.
Brennan’s violated CMS regulations from the earliest point of this interaction because I was not a danger to myself or anyone else when Ms. Brennan first put hands on me, and only when I was touched against my wishes involuntarilythereafter could my behavior possibly been considered dangerous, and yet I was involuntarily restrained for several hours. Even a year later I still suffer an unbearable trauma from this event which my AD, a legal document, was intended to avoid, but it was ignored entirely…
THE FOLLOWING IS THE APS REPORT, WITH NEGATIVE FOR ABUSE…
1. On 11/22/15 DLP received a report indicating PW, alleged victim, was physically abused and unlawfully restrained by a staff member “Annette” at the Vermont Psychiatric Hospital. (Later identified as Annette Brennan, RN)
2. On 11/25/15 this investigator emailed PW to discuss the current allegations and arrange for a face to face interview with another investigator.
3. On December 3, 2015 Investigator Denise Anderson interviewed the alleged victim, PW, at Meadow View Recovery Residence in Brattleboro. PW has been residing at the facility since her discharge from Vermont Psychiatric Care Hospital. PW alleges staff at VPCH conducted an unlawful restraint on her during her stay at the hospital; she has documented this incident on her blog which she indicates she will provide to Investigator Holland-Kelley via e-mail. She stated the incident occurred around 1:00AM on November 18th, the day after her birthday. PW reported she had been “mute” for a few days and asked for a pill of Ativan as it helps her to speak. She stated the staff gave her .5mg and she stated she wanted another.5mg and they refused to give this to her. She stated she was agitated by this denial and a staff member named, Annette, entered the bathroom and grabbed her wrists and had PW’s arms over her head. PW stated she attempted to bite Annette. She stated at that point multiple staff persons entered the bathroom and escorted her out of the bathroom horizontally; each staff person having a limb, and “dumped her onto the mattress in the seclusion room.” PW stated she heard the staff persons conferring because PW had her eye glasses and other items on her person. She stated the staff entered the seclusion room and grabbed these items, including her eye glasses. PW stated this is when they injured her nose (PW has provided a photograph of these injuries). She stated when the staff attempted to exit the room she exited the room with them and the staff escorted her back into the room. PW stated the staff had told her she was not to exit the room but she ignored this command. PW stated it was at this point they used the restraints and secured her to the mattress. PW stated she was restrained for approximately 6 hours; she stated the staff are supposed to assist individuals with range of motion; PW stated she was fearful of developing a blood clot given she was restrained for so long. She stated she did range of motion to her body the best she could as a result. PW stated the staff interpreted this as resistance and considered her to be “flailing.” She stated she did not want to be humiliated by asking to go to the bathroom and then getting restrained again so she stated she opted to urinate in her clothing. She stated Annette “just wanted to take control of things; she wanted to be in control.” She stated she finally agreed to a safety plan and was released from the restraint.” PW does not believe the seclusion was necessary; she believes staff was unnecessarily rough in removing her glasses. PW believes the staff; specifically Annette just wanted to be in control. (Interview with PW,
4. PW meets the criteria of a vulnerable adult as she is over the age of 18 and she has chronic mental health conditions which require she receive assistance with her IADL’s and ADL’s. At the time of this report PW was an inpatient at a licensed psychiatric hospital in Vermont.
5. A review of medical records was done stemming from the noted incident on 11/22/15 involving PW and Annette Brennan, RN. According to the documentation, PW was behaving in an unsafe manner and was considered a danger to herself and others. The staff at VPCH followed hospital policy and procedures to ensure PW’s safety and the safety of the staff. PW was not cooperative with the on duty staff during this time and refused to communicate with them. To ensure everyone’s safety, the staff followed MD orders to assure PW was safe.
6. Further review of the incident report by Annette Brennan RN and other staff members dictate all staff was trying to work to keep PW safe as well as themselves. PW was attempting to kick and bite staff so they had to resort to means to keep everyone safe. Everything done was under the direction and orders of a physician.
7. On 12/21/2015 Mr. Perry stated the VPCH conducted their own investigation involving PW through the JCAH and he would send along the documentation requested for this investigation.
8. On 1/4/16 an invitation to interview letter/request was sent to witness Jennifer Mausukhan, RN with a response due 1/11/16. 9. On 1/4/16 an letter with an invitation to interview response was sent to Annette Brennan with a response date of Jan 15th
10. On 1/7/2016 Ms. Brennan had a telephone interview with this investigator. Ms. Brennan recalls being the nurse in charge on the particular day of the report. She recalls being in the back room with the supervisor and hearing banging going on outside the room. She went out to check and found PW had gone into her bathroom where she had put her mattress on the shower floor thus making her bathroom her safe room. She was trying to slam her door all the while she had 2:1 observation. There were 2 male staff members there. Ms. Brennan decided to put herself between PW and the 2 male staff members because she did not want the staff to be wrongfully accused of anything inappropriate with PW. PW hit Ms. Brennan in the stomach with a notebook and then went to swing at her with her other free arm. It was at this time Ms. Brennan made the decision to ‘take down’ PW and brought her out into the hallway. She had PW carried by 3-4 staff members to the seclusion area. The MD came to assess PW. PW was later searched and as the MD was leaving the room PW tried to attack him. PW grabbed one of the techs around the ankles and Ms. Brennan made the call to put PW in restraints at this time for her own safety and the safety of the staff. PW had received Ativan 1 mg. PRN but the MD did not want her to have any more Ativan. Ms. Brennan said she was checking PW from outside the room. She observed PW move all of her extremities as well as do some ROM (range of motion) to her feet and ankles. She went to check PW up close and PW kicked her in the groin. “I made the decision not to take her out of restraints for ROM”. An employee event was filed. PW screamed extremely loudly later on while still in seclusion. “I was the object of her anger as I was the one making the decision to put her in restraints. She did not just hit me she also hit other staff members and spit on them too. PW was taken out of restraints between 7 and 730pm that evening”. Ms. Brennan denies harming PW at any time.
11. On 1/7/2016 Ms. Mansukhani had a telephone interview with this writer. She stated she was on duty the day of the particular incident noted in this intake report. She stated it was the first time she had met with PW – she didn’t really know her well. She remembered PW going up to the window requesting more Ativan and being told she couldn’t have more (after checking with the MD). Ms. Mansukhani offered her some Melatonin but PW refused that offer. PW became enraged when she inquired which MD had been called and learned it was the MD on call and not her primary MD. (Per policy). PW was lying on the mattress on the floor of the bathroom when nurse Mansukhani went back in to see her. PW was on a 2:1 protocol. PW threw a notebook she had at the wall, not directly at anyone. PW tried to bite Annette (Brennan) and she was kicking. There were a lot of staff members there in the room. They picked PW up and carried her to seclusion area. The MD said not to medicate PW at this time. Ms. Mansukhani stated she went to the other side of the unit at this time because there were only 2 female staff members on duty on the other side and another patient was having a difficult time. PW’s side had 6-7 staff members. When she returned she said she saw PW had restraints on and remembered being surprised and asking what had happened. She recalls asking Nurse Brennan if anyone had checked the restraints on PW. Nurse Brennan told me she had been checking them when PW began kicking her and kicked her in the groin. We offered PW a bedpan which she refused. Ms. Mansukhani got the impression PW was cold and offered her a blanket but PW tried to ‘bite me’ so we removed the blanket. The team decided it was a safety issue so PW did not get the blanket. PW refused to speak to any of us (staff). Nurse Brennan and the doctor said PW had to ‘speak’ a contract to be taken out of restraints which she refused to do. PW later also refused to ‘write a contract with us’. At no time did Ms. Mansukhani observe PW being physically mistreated by any staff members. She observed PW being agitated and struggling with staff. She also observed PW hitting, spitting and kicking staff. “We all tried very hard to meet her needs and get her out of restraints. It didn’t work out that way,” Ms. Mansukhani stated.
Conclusion Statement: Based on the interviews conducted and the evidence reviewed this case will be unsubstantiated. The available evidence indicates A/N/E did not occur. PW was in the midst of a psychotic episode and unable to control her own actions. The mental health staff followed their designated policies and protocols to ensure everyone’s safety at that time.
PLEASE NOTE HOW THEIR STORIES DIFFER FROM EACH OTHERS, AND HOW MINE DIFFERS FROM THEIRS…
(TO BE CONTINUED)
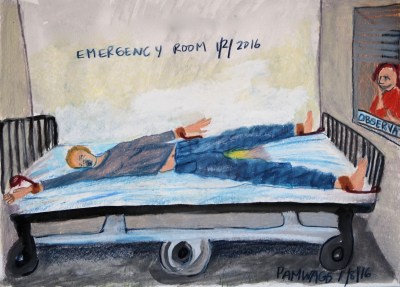
Article about phoebe sparrow wagner’s Emergency Department “care”
Difficult Decision: Will I or Wont I

I went off my psychiatric meds over the course of several months without a problem to speak of, until I was off them for a week, when two things happened. First off the withdrawal dyskinesia (see brief video above) was getting better, but I was beginning to feel, well, nothing, no motivation, no pleasure, no enjoyment in doing anything. I know that many people do not do well on Abilify and hate it, in which case I would say it does little good and to stop taking it. For me, ever since I started taking it in 2006 or so, I have had motivation to start doing and learning art in a way I never felt before. And each time I stop it, no matter how fast or slowly, I go down the hole into no motivation or pleasure in anything. I do not like this situation at all, because Abilify also causes me severe double vision, but but but, I must say that i helps me do things, to finish things, to enjoy the process. I do NOT have any idea why this is, but it has always been so since I started the drug, and I can no longer bear being off it, despite the side effects and disapproval by others. Whatever the damage that years of first generation neuroleptics have done to me, this one drug seems to help me do what I want to do..
.Hate me or not as you will, I cannot bear not taking it. Without it I have no impulse to do art or write, and my life is shit. Is that really what I should be satisfied with?
“Divided Minds” now an audiobook!
13 Things Mentally Strong People Don’t Do
Things Mentally Strong People Don’t Do
BY AMY MORIN
(posted on youbtube by Franque Michele)
Mentally strong people have healthy habits. They manage their emotions, thoughts, and behaviors in ways that set them up for success in life. Check out these things that mentally strong people don’t do so that you too can become more mentally strong.
- They Don’t Waste Time Feeling Sorry for Themselves. Mentally strong people don’t sit around feeling sorry about their circumstances or how others have treated them. Instead, they take responsibility for their role in life and understand that life isn’t always easy or fair.
- They Don’t Give Away Their Power. They don’t allow others to control them, and they don’t give someone else power over them. They don’t say things like, “My boss makes me feel bad,” because they understand that they are in control over their own emotions and they have a choice in how they respond.
- They Don’t Shy Away from Change. Mentally strong people don’t try to avoid change. Instead, they welcome positive change and are willing to be flexible. They understand that change is inevitable and believe in their abilities to adapt.
- They Don’t Waste Energy on Things They Can’t Control . You won’t hear a mentally strong person complaining over lost luggage or traffic jams. Instead, they focus on what they can control in their lives. They recognize that sometimes, the only thing they can control is their attitude.
- They Don’t Worry About Pleasing Everyone. Mentally strong people recognize that they don’t need to please everyone all the time. They’re not afraid to say no or speak up when necessary. They strive to be kind and fair, but can handle other people being upset if they didn’t make them happy.
- They Don’t Fear Taking Calculated Risks. They don’t take reckless or foolish risks, but don’t mind taking calculated risks. Mentally strong people spend time weighing the risks and benefits before making a big decision, and they’re fully informed of the potential downsides before they take action. You may be interested in this too:
14 Things Positive People Don’t Do
- They Don’t Dwell on the Past. Mentally strong people don’t waste time dwelling on the past and wishing things could be different. They acknowledge their past and can say what they’ve learned from it. However, they don’t constantly relive bad experiences or fantasize about the glory days. Instead, they live for the present and plan for the future.
- They Don’t Make the Same Mistakes Over and Over. Mentally strong people accept responsibility for their behavior and learn from their past mistakes. As a result, they don’t keep repeating those mistakes over and over. Instead, they move on and make better decisions in the future.
- They Don’t Resent Other People’s Success. Mentally strong people can appreciate and celebrate other people’s success in life. They don’t grow jealous or feel cheated when others surpass them. Instead, they recognize that success comes with hard work, and they are willing to work hard for their own chance at success.
- They Don’t Give Up After the First Failure. Mentally strong people don’t view failure as a reason to give up. Instead, they use failure as an opportunity to grow and improve. They are willing to keep trying until they get it right.
- They Don’t Fear Alone Time. Mentally strong people can tolerate being alone and they don’t fear silence. They aren’t afraid to be alone with their thoughts and they can use downtime to be productive. They enjoy their own company and aren’t dependent on others for companionship and entertainment all the time but instead can be happy alone.
- They Don’t Feel the World Owes Them Anything. Mentally strong people don’t feel entitled to things in life. They weren’t born with a mentality that others would take care of them or that the world must give them something. Instead, they look for opportunities based on their own merits.
- They Don’t Expect Immediate Results. Whether they are working on improving their health or getting a new business off the ground, mentally strong people don’t expect immediate results. Instead, they apply their skills and time to the best of their ability and understand that real change takes time
____________________________________________
Now I want to share a website where you can find out more about YOU, and why you are the way you are. This website provides a test and a resulting personality profile, which will give you a clue about your ways of being and how and why your interact with others the way you do, as well as your preferences in life for being and doing. http://16personalities.com The test here is free and may be saved as long as you remember to register by putting in your email. The basic profile is free and you can pay for an indepth one but once you get your test results, which is four letter code, much info is available for free on the internet.
Another site, with the official Myers-Briggs test or MBTI, of which the 16 Personalities is a version, and gives much the same results, and this can be found here: https://my-personality-test.com then go to the Personality TYPE test. Now, some of you may be fearful of being labelled but the thing about the MBTI is that it has nothing to do with labels being IMPOSED but any individual’s personal preferences leading to their type being discovered. I found it quite extraordinary, after taking the test a few times, and getting the same results each time, upon reading my profile with an open mind, just how predictive as well as descriptive of my behavior it was. The one thing it never is was prescriptive. It does not tell you what you HAVE to do only what you are likely to want to do or how you are likely to react in any given situation, given your personal preferences in life, and your personality style. Try it, if you don’t like it or don’t respond to it on a visceral level, disregard it!
Cheers, everyone!

VERMONT PSYCHIATRIC CARE HOSPITAL: Today We Will Name Names of the LIARS…and tell all
First of all, I need to make clear that I name the guilty not the innocent here. But I mostly remember the guilty, I wonder why?
As the famed WWII poet Henry Read wrote in his poem, The Naming of Parts:
” Today we have naming of parts. Yesterday,
We had daily cleaning. And tomorrow morning,
We shall have what to do after firing. But today,
Today we have naming of parts. Japonica
Glistens like coral in all the neighboring gardens,
And today we have naming of parts.”
Well, today we have the naming of the liars, and the guilty parties at VPCH, the Vermont State Hospital in Berlin, Vermont, those who either restrained me in 5-point restraints and kept me there for five hour because I could not speak, or colluded to lie about the incident these last two years in order to cover it up and not take responsibility for what happened. And now they have decided to accuse of trying to STAB them…,which is so beyond the beyond that I HAVE HAD ENOUGH!!!
First I will name the Unit D doctor. JOHN MALLOY Jr MD who worked on Unit D at VPCH and who was singlehandedly responsible for a large sheet of paper placed at the front of my chart from the third day I was in the hospital — that is from the the first day he met me, and after he had consulted with the Brattleboro Retreat’s doctor — against my express wishes — by phone only but had not received any official records. This paper had in HUGE LETTERS these words: HOW TO DEAL WITH BORDERLINE PERSONALITY DISORDER…now I do not and did not at any time have symptoms that would have made him think I had such a disorder, except that he had spoken with this monster psychiatrist, Marc McGee from the Brattleboro Retreat, who had diagnosed that secondary Axis II diagnosis within FIVE MINUTES of my — get this! — being forcibly brought into the Adult Low Stimulation Unit by two sheriffs who had not bothered to get a wheelchair but took me by the armpits and dragged me, trussed up like Hannibal Lecter, in leg irons and waist chain and handcuffs and full HOOD over my head and face, across a large parking lot down into the Retreat Basement and up to the second floor where they publicly hauled my helpless body down two long corridors to the ALSA unit before unshackling me…But did Marc McGee ask me why this angered me, I who had been completely compliant on the ride from Springfield and had been hooded the entire time to boot? NO he decided that I SHOULD NOT BE ANGRY so i must have Borderline Personality Disorder…Why? Because HE HATED ME, and his hatred of me meant that I could be abused by him with impunity…
But the thing is, he lied to me, and told me he had not diagnosed this, and it was only later when I found out that he HAD done so right then and there, that I threatened to sue him and to tell the Retreat CEO what he was in the habit of doing to patients he did not like, if he did not remove this designation from my official diagnosis. So he did, he did! When I left, it was not on my discharge summary!
But when Dr Malloy Jr spoke to Dr McGee, did Marc Mc Gee, who ran both Tyler 2 and Tyler 4 units at the Brattleboro Retreat inform him that I was not diagnosed with BPD? No, not at all, he told him the exact opposite, that I had a “long history of BPD” which is utter BULLSHIT and he knows it, Marc told John Malloy Jr that to cover up his own incompetence and John Malloy without bothering to do his own intake and history that VPCH requires him to do, and any thinking on his part, just took that as gospel.
Anyhow, I believe that nothing of what later happened at VPCH would have occurred if the staff had not been primed to abuse me by this sheet of paper that John Malloy Jr MD placed in my chart, instructing them to dismiss me as manipulative and devious and to treat me as a hated patient who needed to be disciplined.
That said, Today we have the naming of names, largely because I just heard from the Vermont Nursing Board that they will not take any measures against the nurse who instigated the Nov 18, 2015 incident of torture. And why? Because the nurse ANNETTE BRENNAN RN, who grabbed me, and had me restrained out of vengeance and kept me in restraints for 5 hours because “she is not to be released until she speaks aloud” (which never happened) was ANNETTE BRENNAN, and she and JENNIFER MANUKHANI RN both know that what they told the nursing board was nothing but a LIE, yet because the nursing board did not know this , and colluded with them, they got away with inventing after the fact something that is not in any part of any chart or debriefing or investigation by the Department of Adult Protective Services, when they investigated the same incident last year, no, nothing was mentioned but suddenly SUDDENLY both nurses manage to remember that I “tried to stab Annette Brennan”?!! Oh, what a load of absolute crap, and if the investigators were anything but idiots who wanted sinecures and not to have to bother to work, they would have done an investigation rather than sitting on their asses. They would have read through the incident in the chart enough to see this. I mean, NOWHERE NOWHERE is this rather critical “event” of my supposedly trying to stab a nurse with a pen ever mentioned (because it never happened) but suddenly it looms as THE ONLY AND PRIME reason why ANNETTE BRENNAN RN that fucking cunt was justified in restraining AND molesting me? Using Dr Joseph LASEK to write the order…
I would have said it took some nerve of those two LYING nurses to collude to make this up out of whole cloth, but they must have known the investigators would not even bother to look to see whether the chart says a word to corroborate this, no of course not. The whole thing was RIGGED to make me look like a assaultive FIEND from the first, when all I ever did was slam doors, NOTHING else, and ANNETTE BRENNAN RN had a hissy fit about it and GRABBED ME because she lost her temper, and Jennifer Mansukhani RN even at the time said, to HER, “WE DON’T GO HANDS ON HERE AT VPCH”, but she had and they did and they TORTURED ME for 5 hours that I cannot forget and will NEVER FORGIVE…
But they got away with LIEs, so I will name names. Annette Brennan, RN and Jennifer Mansukhani, RN TORTURED me and ANNETTE MOLESTED me a helpless patient in 5-point restraints on Unit D at the Vermont Psychiatric Care Hospital on November 18, 2015 with collusion by Drs Joseph Lasek and JOHN MALLOY Jr..
Tomorrow I will post the entire event as I wrote it to the Board, which refused to permit me to testify or to interview me. I wrote it in utter and complete honesty…But they never wanted honesty, they only want to LIE and DECEIVE AND FUCK ME OVER….but REVENGE IS MINE saith the lord as they will learn, and you had better know it!
I also plan to post the pages of my chart and the APS report…I don’t care anymore about MY privacy. FUCK those liars!
Julie Mad Blogger Interview Recorded at Link Here…
EMERGENCY INVOLUNTARY PROCEDURES COMMITTEE MEETING
https://1drv.ms/p/s!AoRt2vNBR5wnhFvBeCFGFVJrs4BZ
https://1drv.ms/p/s!AoRt2vNBR5wnhFvBeCFGFVJrs4BZ
PLEASE GO TO THE LINK ABOVE TO OPEN THE SLIDE SHOW THAT I PRESENTED AT THE EIP COMMITTEE…
On-line Poetry Reading by Pamela Spiro Wagner
Poems start at around minute 9…If you need or want to skip over my reading of the essay. (!)
New Book Launch Announcement!
Interview with Pamela Spiro Wagner, on Schizophrenia and mental Illness in general
Am I opinionated or what? But someone has to SAY these things!!! Peace!
Pam
Donald Trump LISTEN TO THIS: This is My Song…for All the Nations
Art in Progress
I did this chair tonight with drawing Vine charcoal I made in the grill. I peeled wild grape vine then roasted the pieces in wired-together tin box pierced with a nail to let out the gases, for an hour..Inside after that was nice black vine charcoal!

The Second piece is my drawing in progress of which I will try to post a few stages..I have not come anywhere near to finishing it! Nor do Have any idea what it will look like when done!

Paula Caplan is AMAZING: Diagnosis in Psychiatry is BULLshit!

Take a look at this amazing Youtube Video link PLEASE!
