

https://archive.storycorps.org/search/interviews/?q=Phoebe+Wagner
Category Archives: anti-psychiatry

MAD FREEDOM NEWSLETTER

This link is to an article by Vicki Warfield and conversation I had with Vicki in December. I hope you read it and enjoy it!
https://us4.campaign-archive.com/?u=4c0f316156312742402b0121c&id=d0fc84805e

lES MALADIES MENTALES? MENTAL ILLNESS, DOES IT EXIST?
Français then English, paragraph by paragraph.
Pourquoi Il ne faut pas accepter les diagnostics de la Psychiatrie, ou
La normalité n’existe pas!
Bien que les psys parlent des maladies mentales comme si elles vraiment existent, les termes qu’ils utilisent nous montrent que les maladies mentales sont imaginaires et mythiques. Comme tout le monde le sait, les constellations célestes ne sont qu’imaginaire et ce qui constitue Orion pour l’Ouest, c’est quelque chose de différent dans l’Est, qui utilise tout à fait différemment des éléments célestes. Les psys utilisent ce terme aussi, “les constellations”, et ils ont construit leurs constellations d’une manière complètement analogue.
Although shrinks speak of mental illnesses as if they really exist, the terms they use show us that in fact “mental illnesses” are imaginary, the stuff of myths. As everyone knows, the nighttime sky is made up of constellations that are imaginary and that what constitutes Orion for the western world would be meaningless to someone in the east. The Chinese have a zodiac but it is entirely different from ours. Shrinks use this term also, constellations and they have constructed their constellations of mental illness in an entirely analogous fashion.
Parmi des centaines de comportements humaines, la conférence du DSM, composé de psys, a choisi ceux qui vont ensemble (mais pas toujours et pas tout le temps) pour constituer une maladie mentale comme la schizophrénie ou la bipolarité ou la dépression. Comme dans les menus des restaurants chinois on choisit quelque chose de chaque groupe de symptômes — on peut être trop agité ou trop léthargique, ou on peut entendre des voix ou avoir des pensées “différentes” qu’on étiquette les délires, ou on peut faire les choses trop vite ou trop lentement etc— mais en utilisant une formule de leur création, en trouvant ces constellations dans les personnes/ patientes les psys peuvent alors diagnostiquer n’importe qui.
Among the hundreds of human behaviors possible, the committee of the DSM, all shrinks, have chosen those behaviors, (called symptoms but they are really just behaviors ) that go together —but not always and not all the time—to make up a mental illness like schizophrenia or bipolar or depression. Just as we choose food at a Chinese restaurant, or used to, they choose something from certain groups of symptoms — one can be too agitated or too lethargic, one can hear voices or have delusions, or one can do things or speak too fast or too slow etc — but using a formula they created, finding these constellations in the people who visit them, their patients, these shrinks can then diagnose anyone at all.
La chose la plus importante à savoir c’est qu’exactement comme les motifs ou dessins imposés dans le ciel que nous appelons les constellations célestes, ces constellations psychiatriques sont basées dans l’imaginations (assez limitées) des médecins du DSM. Les constellations célestes n’existent que dans les histoires et les mythes grecs, c’est à dire dans l’imagination, et le fait que tout le monde les voit dans le ciel ne dit qu’une chose, c’est que nous avons appris à les voir. Mais nous voyons les constellations psychiatriques et les maladies mentales parce que nous avons appris les voir. Mais elles existent seulement parce que nous les avons accepté sur parole et leur réalité de plus. Nous nous sommes dit, « oui, ce que je vois, c’est une chose réelle cette constellation, cette maladie mentale, et je suis d’accord. » Mais les chinois ne voient pas Orion, n’est-ce pas?
The most important thing to know is that exactly like the imaginary drawings superimposed on the starry sky, psychiatric constellations are also based in the imaginations (perhaps rather limited) of the DSM committee shrinks. The celestial constellations only exist in the stories and myths of the Greeks, which is to say, they are imaginary and the fact that everyone in the west “sees” them only suggests one thing, that we have been taught to see them, these artificial groupings. But we “see” psychiatric constellations, the so called mental illnesses, only because we have also learned to “see” them. Their reality depends on the fact that we have been taught to see them and accept their “reality”. We have said to ourselves, “yes, what I see, it’s something real, this constellation, this mental illness, yes, I agree.”
But ask yourself, do the Chinese “see” Orion? And if not why not?
Et il ne faut pas voir ou accepter l’existence réelle des choses, des constellations ou des maladies mentales. Si on disait que faire les choses vite ou lentement, ce n’est pas un symptôme mais juste une différence humaine, qu’entendre des voix ou que voir les choses imaginaires, c’est un don pas un symptôme, et que ces deux tendances ne sont pas liées dans une constellation pathologique, les soi-disant maladies mentales se révèleraient ensuite n’être rien de plus que de l’imagination, une fantaisie peut être, mais une création imaginaire de psychiatrie, quelque chose qui n’a jamais existé vraiment.
It is not necessary to either see or accept as real these celestial constellations or the psychiatric ones, called mental Illnesses. If we said, for example, that doing things fast or slow, that’s not a “symptom” just a human difference between people, if we said that hearing voices or thinking different thoughts is a gift rather than a symptom, and that these human differences are not somehow inextricably linked in a pathological “constellation”, the so called mental illnesses would reveal themselves to be nothing but imaginary, a fantasy perhaps, but fundamentally an imaginary creation of psychiatry, something that actually never existed.
La prochaine fois je vais discuter la réalité de la souffrance mentale, qui n’est pas la même chose qu’une maladie mentale.
Next time I will discuss the reality of mental suffering, which is not the same thing as a “mental illness.”
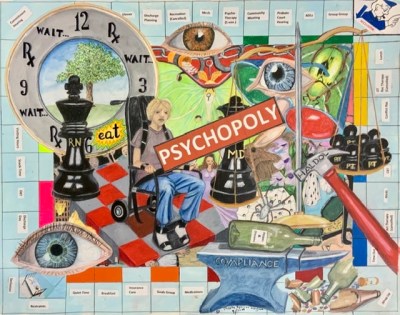
Anti-Psychiatry Art – PSYCHOPOLY
Patient attacked at Vermont hospital
yes, this is the attack I described in yesterday’s post…
Open letter to Elizabeth Warren
Sept 4, 2019
Dear Senator Warren,
I just watched your town hall appearance focussed on climate change, and even though I have been rooting for you and contributing to your campaign ever since you entered the race, I was thrilled to hear you mention both science, your faith in it, and the morass of corruption that characterizes everything in Washington DC.
I know you don’t have a lot of time to read emails, if indeed you read this one, so I will get right to the point.
There is only one group of law-abiding American citizens who can be and regularly are deprived of their civil rights in this country, with utter impunity, and that is the group of us who have been diagnosed with serious mental illnesses, like schizophrenia and bipolar conditions. On the word of a psychiatrist or even in some cases just a masters-degree-carrying “counselor” we can be deprived of our freedom, institutionalized and forcibly drugged for months, even years at a time. Why? Because someone else believes we might be dangerous, even though in fact future violence is notoriously hard to predict, even some will admit impossible to predict.
No one who has committed a crime is kept in prison because of possible future violence, no, what prisons are for, whether you agree with this or not, and I think it is shameful, is to punish, by applying violence to those who HAVE committed a crime. But many, even most of us who have been forcibly hospitalized and drugged have never been violent towards any other person, period. Look at the statistics if you have not already. As those predict, i have been the victim of a violent crime, but never have I been charged with a single incidence of lawbreaking…
Senator, the thing is, if you believe in science, and in rooting out corruption, look at what is going on in psychiatry, and don’t just get the word of psychiatrists, or people who run the so-called mental health system. They either do no know or do not care about the extreme damage the drugs they force on us have done and are doing. They are either completely in cahoots with big Pharma, or they too believe the lies they taught us, that schizophrenia and bipolar conditions are real disease entities, chemical imbalances that such drugs ameliorate if they do not actually amend them. As you may learn, psychiatrists now claim they never said this, that we patients “made them say it.” But this is a lie, and the chemical imbalance lie is still being used on us and the general public.
Psychiatrists as a group do know the truth of what Thomas Insel, former head of NIMH, wrote just a few years ago, that they spent over 20 BILLION dollars in their effort to prove that these things are real neurochemical imbalances, with neuro-anatomic foundations, and in Insel’s words, they “have not moved the needle” on discovering either the cause or any effective treatment.
And yet medication, drugs, are the ONLY treatment that hospitals offer Involuntary patients. In fact, if you are a willingly hospitalized patient, even then such drugs — which shorten the average lifespan by as much as 25 years — are de facto the only treatment. Sure there are “groups” but those who run them will tell you they are just to keep people busy, and are not intended to do anything else.
I am not one of the lucky wealthy people who have been treated voluntarily in posh private hospitals. No, i have been beaten up and tied to a bed too many times to count, which is also involuntary treatment, in public and municipal hospitals, the only ones who took my Medicare and Medicaid, so I know where of I speak…
I could say so much more about this. I am a former medical student, and now an author and artist who was diagnosed and treated, in hospitals and out, for schizophrenia for decades.
The drug companies and psychiatrists lie when they say the drugs work. They do NOT lie when they say that is all they have…indeed it is! But is this right, to lock us up in hospitals because we are different and people claim we might be dangerous for being different? To drug us for life on compounds that drastically curtail our lifespans, and rarely increase our happiness, or our productivity as citizens? No, please see that a resounding NO is the only answer.
And keep us in mind when you become our next president.
Sincerely,
Phoebe Sparrow Wagner

No, you aren’t sick. You have feelings…
A wonderfully explanatory article for my post title.
On my art blog, anti-Psychiatry art
Staff Personality Disorder
I am reprinting this here because it is so true, and because it cannot be located elsewhere on the net, at least not via Google…The author was brilliant but, alas, I can find no name for attribution. A BIG Thank you to Anonymous!
Criteria for Staff Personality Disorder
Personality Disorders
Staff Personality Disorder 601.83
A pervasive pattern of condescension, degradation of others, and controlling behavior beginning by early adulthood and present in a variety of contexts, as indicated by five (or more) of the following:
1. Condescending or degrading use of body language, vocal inflection, and behavior.
2. Presentation of two or more markedly different personality styles based entirely on context.
3. Persistent protection of people in positions of power even if such people have done something unethical or illegal.
4. Employment in one of the “helping professions”, or other situations in which a person has or can secure power over others.
5. Rigidity in application of rules and explanations to other people
6. Persistent or stereotyped use of euphemisms, jargon, deceptive language, and double standards in language
7. Persistent use of degradation, ridicule, and violence, either gratuitously or grossly out of proportion to the situation
Diagnostic Features
The essential feature of Staff Personality Disorder is a pervasive pattern of condescension, degradation of others, and controlling behavior that begins by early adulthood and is present in a variety of contexts.
Individuals with Staff Personality Disorder display condescending or degrading body language, vocal inflection, and behavior (Criterion 1). They may use a patronizing “contaminated” smile, a sing-song voice, or the forms of language use described in Criterion 6. This behavior would be considered patronizing when directed at the average individual.
Individuals with Staff Personality Disorder present two or more markedly different personality styles based entirely on context (Criterion 2). For instance, while dealing with “clients”, while alone, they may be vicious, punitive, and controlling. When dealing with the general public, they may adopt a saintlike persona. It is not at all uncommon for the antisocial behavior of people with Staff Personality Disorder to go unnoticed, even when that behavior extends to torture or murder.
Individuals with Staff Personality Disorder will persistently protect people in positions of power, even if those people have done something unethical or illegal (Criterion 3). This may consist of putting up a “united front” to clients or to the public. People with this disorder will hide or excuse antisocial behavior in others with the disorder. Hiding may take the form of altering logs and failing to report abuse. Excusing may involve character assassination directed toward victims of mistreatment or abuse, or diminishing their credibility in some other way, while making it seem as if the behavior is the only logical response to certain sorts of people. They will also use these techniques of hiding and making excuses, to justify and rationalize their own behavior.
Individuals with Staff Personality Disorder are often employed in one of the “helping professions”, or other situations in which a person has or can secure power over others (Criterion 4). People with this disorder are disproportionately represented among psychiatric technicians, group home workers, home health care aides, social workers, special education teachers, counselors, nurses (especially psychiatric nurses), direct care staff, and institution staff. People with this disorder may also be grammar-school teachers, prison guards, and other professionals in positions of direct power over others. These positions may be either the cause or the result of the disorder.
Individuals with Staff Personality Disorder are rigid when applying rules and explanations to other people (Criterion 5). This, curiously but characteristically, may not extend to others with this disorder. Individuals with this disorder are likely to use a narrow set of rules to understand the behavior of others, particularly clients. They will see most ordinary behavior as manipulative, attention-seeking, or non-compliant. When confronted with something like violence on the part of clients, they will fail to differentiate between malice, self-defense, and frustration at being trapped. This may result in across-the-board application of punishments such as are described in Criterion 7.
Individuals with Staff Personality Disorder may display persistent or stereotyped use of euphemisms, jargon, deceptive language, and double standards in language (Criterion 6). They euphemistically refer to others as special needs, challenged, or consumers. They prefer jargon to ordinary language, and describe the behavior of others using clinical and psychiatric jargon, often loosely adding such jargon into everyday conversation, e.g. saying that someone they dislike has a Borderline Personality Disorder. They use deceptive language, for instance referring to prisons as hospitals and violence as treatment. They use double standards in language, e.g. referring to themselves as getting bored but to clients as going off task. They may apply certain words in a stereotyped fashion, repeating over and over that others are non-compliant, attention-seeking, manipulative, or playing games, without apparent regard to context or motivation.
Individuals with Staff Personality Disorder display persistent use of degradation, ridicule, and violence, either gratuitously or out of proportion to the situation (Criterion 7). Degradation may take the form of degrading language such as “retard” or “psycho”, denial or pathologization of the existing identity or roles of others (for instance telling someone that thinking he is a writer is a delusion of grandeur), treating people like children, or assigning humiliating tasks. More advanced forms of degradation involve using elaborate methods to thoroughly confuse a person’s sense of reality or self on all levels. Ridicule might include laughing at the aspirations or humiliation of clients, or laughingly dismissing their communication or behavior. Violence includes physical or sexual assault, mechanical restraints, chemical restraints, and solitary confinement. These things may be undertaken gratuitously, on a whim, as a result of boredom or frustration. They may be out of proportion to the situation, such as restraining someone for making eye contact with staff. These things are often justified using the means described in Criterion 3.
Associated Features and Disorders
Individuals with Staff Personality Disorder may have a tendency to take care of people who don’t need taking care of, or imposing their idea of care onto other people regardless of context or other people’s wishes. They may have a tendency to rationalize their own behavior in terms of helping others and be apparently unable to see their victims as fully human. They can be highly manipulative, especially to those they regard as inferior. Staff Personality Disorder may be associated with Stockholm syndrome and complex post-traumatic stress disorder in individuals who have been subjected to abuse by people with the disorder. Thus, a significant minority of people who are in institutional situations may develop features of this disorder or the full-blown disorder. Staff Personality Disorder is sometimes seen in the prodromal stages of developing full-fledged Psychiatry Disorder. Non-disabled children who participate in “Circle of Friends” and other helping-based friendship programs are more likely than other children to develop Staff Personality Disorder by adulthood, as are children who have been raised to be caretakers to disabled siblings or parents. People who go into the “helping professions” or who work in institutions are at high risk of developing Staff Personality Disorder, even if they have shown no signs of it in the past.
Specific Culture, Age, and Gender Features
The pattern of behavior seen in Staff Personality Disorder has been identified in many settings around the world, but is especially common on the top end of unequal power situations. Children imitating adults may transiently show signs that seem to point to Staff Personality Disorder where none is present. In the past, it seemed that Staff Personality Disorder was more prevalent in females, but it is now accepted that due to cultural pressures, it can present differently in males and females.
Prevalence
The prevalence of Staff Personality Disorder is estimated to be about 5% of the general population, about 80% among individuals who work in outpatient settings, about 95% among individuals who work in inpatient settings and other total institutions, and about 20% among inpatients and other people who experience prolonged abuse at the hands of people with Staff Personality Disorder.
Course
While there is considerable variability in the onset of Staff Personality Disorder, there is almost no variability once it becomes entrenched in a person’s identity. The most common pattern is that a person seeks a job in any of a number of “helping professions” and is gradually molded into the behavior patterns that typify Staff Personality Disorder. There is a window of opportunity in acclimation to these behavior patterns, in which a person may still have the insight to quit their job or resist further indoctrination. Once these behaviors become entrenched, they are self-justifying and rarely respond to reason or therapy. This is enhanced by the fact that many people with Staff Personality Disorder spend a lot of time socializing with other people with Staff Personality Disorder. A minority of individuals, when presented with the evidence of the harm they have caused to others with their behavior, truly become cured of Staff Personality Disorder, although literature indicates this requires constant vigilance to avoid falling into their old behavior patterns. Some people with Staff Personality Disorder acquire a disabling condition or another mental disorder and recover after learning what it is like to be subjected to the behavior of people with Staff Personality Disorder, but others will maintain their staff identity even within the inmate role.
Familial Pattern
Staff Personality Disorder is about five times more common among first-degree biological relatives of those with the disorder than in the general population. There is also an increased familial risk for Psychiatry Disorder.
Differential Diagnosis
Staff Personality Disorder often co-occurs with Psychiatry Disorder, and when criteria for both are met, both should be diagnosed. In instances where it is related to the development of post-traumatic stress disorder or other trauma-related disorders, it should be diagnosed in addition to those disorders with a notation that they are connected.
Other Personality Disorders may be confused with Staff Personality Disorder because they have certain features in common. It is, therefore, important to distinguish among these disorders based on differences in their characteristic features. However, if an individual has personality features that meet criteria for one or more Personality Disorders in addition to Staff Personality Disorder, all can be diagnosed. Although Histrionic Personality Disorder can also be characterized by manipulative behavior, Staff Personality Disorder is distinguished by condescension. Paranoid ideas or illusions may be present in both Staff Personality Disorder and Schizotypal Personality Disorder, but in Staff Personality Disorder these ideas are limited to concerns about the behavior of those under the person’s control (often inmates). Although Paranoid Personality Disorder and Narcissistic Personality Disorder may also be characterized by an angry reaction to minor stimuli, the reactions in Staff Personality Disorder have to do with specific situations related to the staff role and distinguish these disorders from Staff Personality Disorder. Although Antisocial Personality Disorder, Borderline Personality Disorder and Staff Personality Disorder are all characterized by manipulative behavior, individuals with Antisocial Personality Disorder are manipulative to gain profit, power, or some other material gratification, the goal in Borderline Personality Disorder is directed more toward gaining the concern of caretakers, and the goal in Staff Personality Disorder is to maintain control over a specific person or group of people. Also, while individuals with Antisocial Personality Disorder rarely show remorse for their antisocial behavior, individuals with Staff Personality Disorder make heavy use of specific rationalizations to justify their behavior to their conscience. However, some people with Antisocial Personality Disorder may have co-morbid Staff Personality Disorder and both should be diagnosed in that case. Personality Disorder can further be distinguished from other personality disorders by the typical pattern of protecting others with the disorder and persistent use of euphemisms and jargon to describe one’s actions.
Staff Personality Disorder must be distinguished from Personality Change Due to a General Institutionalized Condition, in which traits emerge solely in the institutional environment due to the direct effects of people with Staff Personality Disorder on an inmate’s behavior.
It also must be distinguished from Factitious Staff Syndrome, in which a person without Staff Personality Disorder masquerades as a person with Staff Personality Disorder in order to assume the staff role and effect change for the better for those under the power of people with Staff Personality Disorder. Factitious Staff Syndrome does not qualify as a mental disorder, but individuals practising it unwarily may develop Staff Personality Disorder.
Judge Rotenberg : TORTURE, nothing more needs to be said

Flynn Center Art Show for persons with disabilities
A

My picture NOT WAVING BUT DROWNING will be in this show. Click on link to see full color information
Continue reading Flynn Center Art Show for persons with disabilities

What Really Happened On W-1 in New Britain Hospital’s Psychiatric Unit in 2014…
I remember names…some of them. For instance, the short, chubby, blond nurse, who was worried about her weight and who was so instrumental in torturing me? Her name was Debra. And the head nurse who seemed so oblivious to the fact that her policies were indeed torture, even though she admitted that she expected the guards to inflict pain on patients when “escorting” them to seclusion in order to “subdue them faster” as she put it to me, openly. Her name was Barbara, and even though I was horrified by things she told me, I believe that she was innocently deluded and believed in her job, did not mean to be mean, not the way Debra seemed to, and honestly wanted the best for her patients. But let me start at some beginning which is to say, anywhere at all, and give you an idea of what I am talking about.
I have written in multiple places and on many occasions about what happened to me at New Britain Hospital (aka Hospital of Central Connecticut on Grand Street in New Britain) and I do not want to go into the whole thing here. All you need to do is search on the subject of Michael E Balkunas at this blog and you will get most of the gory details. That said, much that happened has never been told not even here. For instance, that Debra was the nurse who in a sadistic impulse and in an apparent fit of frustration, decided to have the security guards strip me naked when she was secluding me for some unknown (and always unnecessary) reason yet again…as they did nearly daily at W-1 in New Britain Hospital in May 2014….that it was Debra who was directly responsible for this I have never stated. But I remember her name clearly, and her face….And the fact that after she did this the second or third time she went on leave for several days, and when she came back told me she had almost quit her job.
I was momentarily cheered because I thought perhaps she had had some serious regrets about what she’d done to me. I asked her, Was it because of me? I thought she would tell me yes. She looked at me, and nodded, then said, “Because you are such a challenging patient.” Huh? I looked at her, and saw no remorse, no regrets only residual anger and scorn…and a certain unrepentant rancor that I had “made her do what she did.” Clearly she felt that I was to blame for her behavior, that I was to blame in general and that it was all justified.
But to get back to what happened. After she had me stripped naked by four male guards, after I loudly and vociferously protested being left alone in that freezing seclusion cell for I never knew how long, I began mildly hitting my head on the wall in protest. They threatened to four-point me and then they came barreling back in and threw me onto a restraint bed. The thing is, I knew, completely naked, I could not take the cold in that seclusion cell. But if they restrained me they would HAVE to cover me with something, and at the very least I would not freeze to death in that frigid cell for an indefinite number of hours…But when they came for me, they grabbed me and angrily threw me onto a gurney, even though I put up no resistance, spread-eagled my legs, deliberately exposing my private parts, and shackled them to the corners of the gurney with my arms pinioned above my head until I shrieked in pain even as they laughed. Then they held me down, gratuitously I might add, since I was already restrained, compressing my neck and chest, in order to give me the usual three-injection cocktail of punishment drugs — Haldol, Ativan and Benadryl — forcibly slammed into my buttocks. All of this done to me while I was naked and immobilized in four point restraints. Then fearing that they would leave me alone there, freezing cold, I screamed for them to cover me. With a look of disgust, someone threw a draw sheet over me, but no more.
The charge nurse came in for my “face to face” interview to see that all was “proper” and she visibly and audibly shivered, but refused me a warm blanket, or any at all, due to “safety concerns.” Then she left with the rest of them and turned off the intercom, so “we won’t have to listen to her scream.” They closed the door behind them, leaving me all alone behind a metal cell door that did not even have an observation window in it.
I screamed from the base of my lungs as deeply and as loudly as I could for as long as I could last. No one took mercy on me or brought me water or a blanket or spoke to me the entire time. Only when, exhausted, I finally lapsed did they relent and ask, from outside the door, “can we turn the intercom back on? She is quiet now…” And apparently got assent for that… Because eventually I heard someone flip a switch but nothing more.
After I was released, the next day, I told the unit director, Dr Michael E Balkunas what they had done to me, and he must have recognized the egregious nature of it because his response is telling. Instead of dismissing it as not so terrible, he said: “They would NEVER do such a thing as that in my hospital. You are a liar!” So he saw how awful it had been, what they had done to me, he just refused to acknowledge it had happened, and that he did not in fact what his staff were up to. But I was never in fact the liar he believed me to be. His stock answer to everything he did not want to see or believe was routinely that I was lying, but this was not true, and he was so sickeningly dismissive of the truth that I did not wait to listen to more this time. I was so wiped off the map by his response that I got up and walked out of the interview room and did not bother with him from then on…I KNEW I was never a liar, and that in actuality it was the STAFF who lied all the time, but telling Balkunas that would have done no good. He wanted to believe what he wanted to believe and nothing i said got through to him from day one…So I thought, so why bother ? WHY BOTHER. Balkunas wanted to murder my body and my spirit, and I could not let him succeed. He could imprison my body in his hospital, but i was damned if i would let him get my spirit. FUCK HIM!
But Dr Balkunas, Michael, you did not in point of fact know what went on at W-1 ever, nor at the ER, when you were there. Abuse was rampant because you encouraged it to be…and you never cared much what they did to achieve “order” so long as it was “quiet” when you were around. So you gave tacit assent to the tortures that they inflicted, and you likewise tacitly approved the very behaviors that you told me would “never happen on your watch”…Yeah? Well, I feel certain that if they behaved as they did towards me, they had done it before me, and did so to others after I left as well…and they continue to inflict these things on patients to this day.
I will leave it there. Your unit staff and you too, Balkie, are Out of control, and deserve, as my Obama post notes, to be CLOSED down for good.
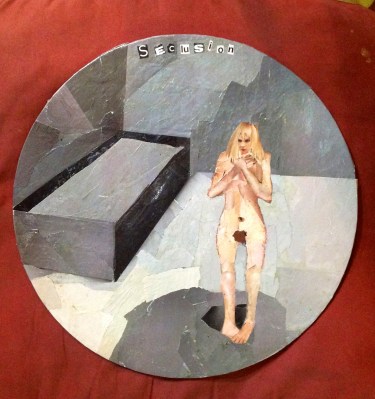
The other day I made this little polymer clay figure to illustrate what Debra did to me.

It blew me away and I could not sleep all night the night I made her….Until Wendy and I decided to heal her, and perhaps heal me, from the experience, First, talking to the figure in the little bed calmly and with compassion, we covered her with a thick cotton blanket. That brought me some relief as I no longer felt chilled. Then we took off the restraints, which despite being made of polymer clay actually slipped right off, and we brought her arms down to her sides so she could sleep in comfort. By the time we were through I felt immensely better.
Neither of us could even imagine treating another human being as Balkunas had had me treated on numerous occasions by routine.
