whatever the season, forgive it its various assaults
— floods, gales, storms of ice —
and forgive its changing; for its vanishing act,
stealing what you love and what you hate,
indifferent, forgive time;
and likewise forgive its fickle consort, memory
which fades the photographs of all you can’t remember;
forgive forgetting, which is chaste and kinder
than you know; forgive your age and the age you were when happiness was afire in your blood
and joy sang hymns in the trees;
forgive, too, those trees, which have died;
and forgive death for taking them, inexorable as God; then forgive God His terrible grandeur, His unspeakable Name
forgive, too, the poor devil for a celestial falll no worse than your own.
When you have forgiven whatever is of earth, of sky, of water, whatever is named, whatever remains nameless
forgive, finally, your own sorry self, clothed in temporary flesh,
the breath and blood of you already dying.
Dying, forgiven, now you begin.
by Pamela Spiro Wagner in “We Mad Climb Shaky Ladders” (Cavakerry Press 2009) also featured in “Divided Minds: twin sisters and their Journey through schizophrenia.”
When I was at New Britain General Hospital in the spring of 2014, the security guards stripped me naked and left me in the freezing and barren seclusion room…This is a depiction of a younger woman largely because no one gives a damn about what happens to a 61 year old woman anywhere..but the seclusion room is pretty danged accurate.
Dr Geuss: Life-size Papier Mache Goose made for Vermont Northeast Kingdom’s Human Services
Dr Geuss: Papier Mache life-size goose made for Vermont’s North East Kingdom’s Human ServicesSea Turtle in Turquoise and Blues…Water soluble oil pastel c. 7 inches by 6 inches
I want to reblog this brilliant post by Anne C. Woodlen and then i will add my own editorial comments if i can in a later post or edit. In the meantime, i think it speaks for itself and says just about what i would want to tell a lot of young people newly diagnosed with bpd or did or add or even bipolar disorder and getting on disability, preparing for a life “in the system” – it sucks and it isn’t worth it unless you are floridly psychotic. And even then, don’t believe what they tell you about antipsychotic drugs. There ain’t no such medication, only sedatives that may or may not quiet things down temporarily. The only way out is through, if you can do it with a wise and caring guide and community. Don’t get stuck as i am, on multiple antipsychotic drugs, addicted to them so that getting off them only means you get more psychotic than ever. Psychosis need not be a lifelong problem, but it certainly will be if you keep taking high doses of the drugs and never explore other options.
My name is Dustin and I live in Michigan. When I was seventeen years old my mother put me in a psychiatric hospital called Forest View. The abuse I felt violated me to the core! I felt like I was being raped having to submit to all the rules, the bullying and the emotional abuse. To have your dignity removed when you are an innocent patient and just want genuine, kind, gentle care, and get unprofessional jerks who you can tell are fake and just care about getting paid is a horrible experience. If anything it only caused me more traumas with the trauma that I already had. I am now twenty-two years old and live on disability while also living my life as a hermit because now I am afraid of people due to the awful treatment I endured. I was diagnosed with Borderline Personality Disorder by a REAL…
Pam with unfinished paper mache goose, TooGoose Lautrec….
Across the driveway live some great people…
Kitchen and work area in cottage
More of Work area and art areaStephanie is “gods gardener” or so I call her!Steffie at the state park
As my time here comes to an end, I will miss it and my neighbors terribly., I don’t know what I will do without them, and Lydia my wonderful companion. Returning to Connecticut with its horrible hospitals and indifferent treatment just feels like a disaster waiting to happen. I want to move to Vermont but I don’t know how I can make that happen. I have felt amongst friends everywhere here, but isolated completely for years in CT, despite my lovely dear friends there, I wish I could bring them all up to VT with me!
This video is pretty sickening and difficult to watch. However it is brief and necessary, if you care about what the police are doing tp everyday citizens in this country… (Need I mention that Eric happens to be African American, which I believe was significant in his treatment, just as a mental illness would have been or other supposedly extraneous factors…
Connecticut Hospitals Responding to Psychiatric Restraint Numbers
By DAVIS DUNAVIN
View Slideshow
Pamela Spiro Wagner and her art.
Davis DunavinWNPR
1 of 3
“They don’t want you to get out. They pull [restraints] as tight as possible to the sides of the bed.” Pamela Spiro Wagner
Pamela Spiro Wagner’s apartment is full of art she’s made while in psychiatric care. One piece dominates the room. It looks like a painting at first. It shows a threadbare seclusion room and a restraining bed.
“That’s made of Vogue magazines. If you look at it, you’ll see there’s a little label of Prada leather on the leather restraints, which was done on purpose,” Wagner said. She made it while alone in a hospital seclusion room. The magazines were the only art supplies she had.
Wagner has schizophrenia. She’s been in and out of Connecticut hospitals for decades, and she knows what it’s like to be restrained. “They use leather, or rubber, or plastic, or whatever restraints that they wrap around your wrists, usually tight because they don’t want you to get out. They pull them as tight as possible to the sides of the bed,” she said.
Wagner was put in four-point restraints. That means each limb is bolted to the bed, and she said she’s stayed there for nearly a day at a time. “I would just scream from the base of my lungs,” she said, “like the screams that if you had any heart, your heart would break if you heard me scream.”
“Restraint is Pretty Traumatic”
Patricia Rehmer, Commissioner of the Connecticut Department of Mental Health and Addiction Services, said the department has cut down on restraint since receiving a federal grant in 2008. “We know,” she said. “The literature is clear; the clients are clear. Seclusion and restraint is usually a pretty traumatic event. If we had our way, there would be no seclusion and restraint. We’d love to get to zero, but that’s not always possible.”
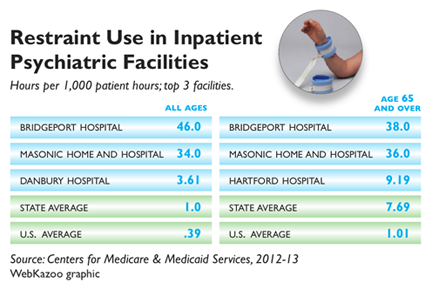
Credit WebKazoo / Connecticut Health I-Team
The Department of Mental Health and Addiction Services oversees state hospitals in Bridgeport, New Haven, Hartford, and Middletown. Rehmer said that because patients stay longer at state hospitals, doctors and nurses have more time to work with them on ways to avoid restraint. “Frankly, there are differences between our hospitals, our hospital beds, and general hospital beds, for example,” she said.
Restraining or secluding patients used to be commonplace in psychiatric facilities, but ten years after a series of deaths nationwide, there’s been a push to lessen the time patients spend restrained. Federal data released earlier this month showed that Connecticut’s rates of restraint are still high compared to most of the country – more than double the national average. The state ranks eleventh nationwide, and third for use of restraints among the elderly.
Connecticut Institutions Adapt
Bridgeport Hospital topped the list statewide. The hospital has a large geriatric unit, and the numbers were high for elderly patients.
“We realized about a year and a half ago that we were really having a problem,” said Ryan O’Connell, Bridgeport Hospital’s vice president of performance and risk management. He pointed out that the numbers only go up to the middle of 2013, and said that the hospital started changing its practices since then. “It was much more common for us to go to some type of restraint,” he said.
O’Connell said the image of the barren room and four leather straps is all wrong at Bridgeport. They’re mostly trying to keep patients with dementia from wandering off and into danger. “I think it’s really important,” he said, “that nobody thinks that we were tying people down [by their] hands and feet.”
Bridgeport is moving toward something called comfort rooms, with colorful wallpaper, toys, games, or comfortable furniture. They’re becoming common alternatives in a lot of institutions, like Connecticut Valley Hospital in Middletown — a state hospital that cut back on using restraints by about 88 percent in the past decade.
In 2002, a patient died after being restrained at CVH. The hospital conducted investigations after the death, but Director Charles Dike said they’d already decided to make a change before it happened. “Our target is to make sure we use it as sparingly as possible, only when it is absolutely necessary, and that we discontinue it as quickly as possible,” he said.
CVH started using comfort rooms years ago. Dike said that instead of putting a patient in restraints, they try to encourage a patient to spend a little time alone doing something relaxing. He said, “If somebody says to me, when I’m not doing so well, I like to go into my room and play music, and that helps me calm down…” He said that nurses will remember, and bring it up if the patient starts to lose control.
Dike doesn’t expect to stop using restraints. He said there will always be outliers — patients who come straight from emergency rooms and prisons.
Ellen Blair is the nurse director at Hartford’s Institute of Living, which is part of the Hartford Hospital system. Figures for 2013 show Hartford Hospital restrains patients at a little over the state average, but she said they’ve cut back since then thanks to new training programs and more comfort rooms.
Blair said that when a patient does go into restraints, they’re looked after. “I personally go and make sure I know that patient,” she said. “We all talk about it at least every couple of hours, because we don’t want to keep it going any longer than we have to.” She said patients aren’t left alone, and that restraint is only used as a last resort when patients are dangerous to themselves or others.
“Every day,” Blair said, “we come here thinking, okay, we’re going to have a good day. We’re going to prevent people from getting agitated and having to go to that level.” Restraint, however, remains a last resort these hospitals said they don’t plan to take off the table entirely.
3 COMMENTs
Comment 3
Pamela Spiro Wagner:
Dear John Dankosky,
Thanks for posting both my earlier comments.
I must tell you that I still think your piece assiduously avoided saying anything that implicated Hartford Healthcare, and ultimately portrayed all the hospitals (NPR sponsors naturally) in a golden light. When Ellen Blair, the IOL nurse manager, stated that “every two hours” the Hartford Hospital Institute of Living nurses discuss any patient in restraints did you really recognize that this means a given patient remains in restraints? NO patient should still be in restraints after two hours, it just isn’t necessary. You should be aware that when a patient is mechanically restrained it also means that he or she has been injected in the buttocks with chemical restraints or emergency medications (though staff will never call the forcibly injected drugs by such a name as a “chemical restraint”). This is a given, but it means that the patient is almost always asleep after two hours or most certainly calm, if they were indeed truly and emergently dangerous in the first place. At the IOL, however, if he or she has not spoken the verbal “Uncle!” that is required, the nurses will not take restraints off. How can you say “I promise to stay calm…” yadda yadda if you are asleep? Nevertheless, the strict CMS guidelines are that restraints must be removed as soon as a patient is calm and no longer a danger to self or others. It should be obvious that once a drug has sedated a patient the patient is not an imminent danger to anyone. (It might be argued that both “emergency medication” and restraints are overkill and that one OR the other should be used, never both.)
“Imminent” is the operative word in the criteria for restraints: a person must pose an “IMMINENT danger to self or others.” In my case I was never really a danger to anyone. I was simply a PIA…and the staff as much as said so. If you have read my other comments below, you will have understood that even the Centers for Medicare and Medicaid (CMS) as well as SAMHSA understand that seclusion and restraints are almost never necessary, despite what the doctors and nurses told your reporter and what you summarily reported as true. As I quoted from the document put out by SAMHSA in my comments, both restraints and seclusion are usually used in retribution or as the result of a power struggle which the institution necessarily “wins” when these methods are chosen…but are rarely used as the result of emergency situations.
I suspected that this was the sort of report that you would do. Yes, you gave me a kind of voice, or at least two sentences worth, about the trauma of restraints, but you never named the institutions that restrained me so viciously, though I did name them over and over in my interview. And you gave a much greater voice to those institutions attempting to whitewash their current practices… You did not actually investigate whether or not they do as they say. Or even whether what they say they do is in fact as benign as it is cracked up to be.
Think, think, think…Ellen Blair casually mentioned ”every two hours a person remains in restraints.” What, for four hours, six hours, 19 hours as she and her cronies kept me in restraints???…WHAT IS SHE THINKING???? NO ONE SHOULD BE IN RESTRAINTS SO LONG unless something brutal is going on. Even at New Britain General I was always taken out of restraints after 2 or 3 hours. Why? Because under the influence of the medications, I got sleepy and did as I was told…Yes, even though they were brutal they never kept me restrained longer than that. As soon as the requisite hours of punishment were up, I was allowed out. Period.
Hartford Hospital’s Institute of Living should be ashamed of itself, restraining and keeping someone in restraints when asleep and then re-injecting them with medication in order to put them BACK to sleep while still in restraints as they did to me time and time again.
You know, I would give you permission to see my entire chart from my 2013 Hartford Hospital stay, if you ever wanted to investigate these charges and find out whether what I say is true. I believe in fact that they do this sort of thing regularly at the IOL Donnelly building. I do not believe I am the only one. That is the problem, you see. This is a practice of theirs. I am NOT unique and was NOT singled out but rather treated brutally because this is how they do things at the Institute of Living and from what I gather from Ellen Blair, they are still doing it.
Whether NPR cares enough to hear or report what is really being said beneath the pretty words, or to find out the truth about what goes on inside these hospitals, I do not know…I tried to inform Davis Dunavin. I do know what happens because I have been inside many times, and it has happened to me. But you did not report even a smidgen of what I told him. So much for reporting the facts or even a portion of the whole truth.
I was restrained at Hartford Hospital’s Institute of Living in January 2013 for 19 hours at a time several times during a mere 3 week stay. And why? They told me repeatedly it was because “You do not follow directions.” The SAMHSA and CMS knows that restraints and seclusion are almost NEVER necessary. I quote from a SAMHSA publication: “Studies suggest that restraints and
seclusion can be harmful and is often re-traumatizing for an individual who has
suffered previous trauma…
“Further, there is a common misconception that seclusion and restraint are used only when absolutely necessary as crisis response techniques. In fact, seclusion and restraint are most commonly used to address loud, disruptive, noncompliant behavior and generally originate from a power struggle between consumer and staff. The decision to apply seclusion or restraint techniques is often arbitrary, idiosyncratic, and generally avoidable.
“Moreover, some studies indicate that seclusion and restraint use leads to an increase in the behaviors that staff members are attempting to control or eliminate.”
When restraints and seclusion are used, certainly in my case, as my Psychiatric Advance Directive CLEARLY indicated, my symptoms always get worse, I regress to primitive behaviors and things go from a situation that might have been ameliorated with ease to something that only traumatizes me terribly (I already have PTSD on top of schizophrenia) and should traumatize any nurse who still has a heart.
When I heard via this broadcast Ellen Blair APRN say how much care they take at the IOL to avoid restraints there, I could have laughed. If so, why then would they restrain me for hours day after day for as little as tossing half a graham cracker at the wall in frustration. Indeed, if it took as few as a single nurse to put me, passive and non-resisting, into four point restraints, how could it possibly be “necessary,” except to teach me a lesson or punish me? But in fact, it was punishment most of the time, and nothing more. There was a power struggle that developed between meand Amy Taylor
MD, and she was determined to show me who was in charge. That was the problem. The only way I got out was because she took two days off, and a kindly substitute doctor took me out of restraints and asked me if I wanted to go home. I said yes,PLEASE, and that was that.
Comment 2:
I would like to add that the image of the concrete barren seclusion room and leather restraint cuffs rather than being “dead” is alive and well in many CT hospitals. I was at the Hospital of Central Connecticut, the former New Britain General Hospital in May and June of this year, 2014, and their seclusion rooms were worse than a supermax prison cell. Literally. There were NO amenities there as there are in a supermax cell, no toilet, not even a bedpan. Just a concrete bed, with a rubberized mattress. And when they considered me “dangerous” to myself, they stripped me of all my clothing and left me naked, despite my desperate pleas for a blanket for protection against the air-conditioning which was always on full-bore.
Even the doctor, who put me there time after time, told me that “the nurses would never leave you without covering or a blanket.” He did not believe me when I told him that in fact this was their regular practice. Moreover, hospital security guards were the ones to strip me forcibly and then four-pont me still naked to a bare mattress, only covering me with a sheet when I begged for one.
It was the most horrendous experience I have been through since, well, since the Institute of Living in 2013. And they did this on multiple occasions, despite KNOWING from the first that I had come in with PTSD in addition to schizophrenia and that I had an Advanced Directive that gave clear instructions about what helped me calm down and how best to treat me in order to avoid escalating situations. What is worse, the policy at HOCC is that nurses are NOT permitted to touch or lay a finger on any patient,…ONLY security guards do that. And they grab any patient willy nilly, usually with the deliberate intent to inflict pain, as the nurses told me, because if they cause pain the patient will comply. This is, excuse me, crazy! There is something very very wrong with this picture…but the staff at HOCC was so encultured with their way of doing things, that they had lost sight of how wrong it was. It simply didn’t occur to them that guards hurting patients might be not only morally wrong but just plain ineffective if they wanted to help someone get better.
But maybe I am the one who is “nuts” thinking that HOCC staff cared about anyone “getting better” — maybe they just did their “jobs” and didn’t give a hoot in hell whether the guards deliberately injured patients or not, so long as the “job” whatever it was got done…
Avenging Angel in Gouache – Abstract approximately 7 by 8 inches
Lots to say about the situation I am in up here in Vermont, where my assistant, the person hired to help me and make sure things go okay turned out to be a common criminal. But I am too tired and worn out by having to deal with the mess left in her wake to write about it. Suffice it to say that she stole my debit/credit card number and racked up multiple charges, was apparently drinking even in the mornings without my knowing it, and driving me at the same time. She had a hand bag full of narcotics not all of them prescribed to her, but even if they had been, what was she doing, taking narcotics and drinking and driving?!
Things were even worse than that, but as I said, I am exhausted and cannot go into it all now. Needless to say, she has been fired and is gone, is out of here…But she has left a mess and misery in her wake all around. What a mess maker! And I think she was the one who was stealing from me all the while last winter when I had people staying with me to prevent a hospitalization…Why did I once trust her implicitly? Where do I find these people and WHY do I trust them at all?
I should have known something was wrong when I saw her handbag full of Percocet and Xanax and VIcodin and fentanyl patches etc. It was ridiculous…and then to have her buy a case of beer? But I thought “well, a beer once in a while is harmless.”…I didn’t know she was drinking at breakfast and also while driving…I am such a dimwit!
Sometimes the voices are so loud, you just have to scream…
Novel ‘Avatar Therapy’ May Silence Voices in Schizophrenia
Deborah Brauser
July 03, 2014
LONDON ― A novel treatment may help patients with schizophrenia confront and even silence the internal persecutory voices they hear, new research suggests.
Avatar therapy allows patients to choose a digital face (or “avatar”) that best resembles what they picture their phantom voice to look like. Then, after discussing ahead of time the things the voice often says to the patient, a therapist sits in a separate room and “talks” through the animated avatar shown on a computer monitor in a disguised and filtered voice as it interacts with the patient.
In addition, the therapist can also talk by microphone in a normal voice to coach the patient throughout each session.
In a pilot study of 26 patients with treatment-resistant psychosis who reported auditory hallucinations, those who received 6 half-hour sessions of avatar therapy reported a significant reduction in the frequency and volume of the internal voices ― and 3 reported that the voices had disappeared altogether.
“Opening up a dialogue between a patient and the voice they’ve been hearing is powerful. This is a way to talk to it instead of only hearing 1-way conversations,” lead author and creator of the therapy program Julian Leff, MD, FRCPsych, emeritus professor at the Institute of Psychiatry in London, told meeting attendees.
Dr. Julian Leff
“As the therapist, I’m sharing the patient’s experience and can actually hear what the patient hears. But it’s important to remind them that this is something that they created and that they are in a safe space,” Dr. Leff told Medscape Medical Newsafter his presentation.
Two presentations were given here at the International Congress of the Royal College of Psychiatrists (RCPsych) 2014 the day after the study results were released in the print edition of Psychosis.
Regaining Control
According to the investigators, 1 in 4 people who hear phantom voices fail to respond to antipsychotic medication.
Dr. Leff explained that this program started a little more than 3 years ago, after he had retired “and could start thinking clearly again.” He had been interested in the phenomenon of phantom voices for more than 40 years.
“Our mind craves meaningful input. That’s its nourishment. And if it’s deprived of nourishment, it pushes out something into the outside world,” he said. “The aim of our therapy is to give the patient’s ego back its mastery over lost provinces of his mental life.”
The researchers used the “off-shelf programs” Facegen for the creation of the avatar faces and Annosoft LIP-SYNC for animating the lips and mouth. They also used a novel real-time voice-morphing program for the voice matching and to let the voice of a therapist to be changed.
In fact, Dr. Leff reported that one option the program provided changed his voice into that of a woman.
After a patient chose a face/avatar from among several options, the investigators could change that face. For example, 1 patient spoke of hearing an angel talk to him but also talked about wanting to live in a world of angels. So the researchers made the avatar very stern and grim so that the patient would be more willing to confront it.
Another patient chose a “red devil” avatar and a low, booming voice to represent the aggressiveness that he had been hearing for 16 years.
For the study, 26 participants between the ages of 14 and 74 years (mean age, 37.7 years; 63% men) were selected and randomly assigned to receive either avatar therapy or treatment as usual with antipsychotic medication.
The length of time for hearing voices ranged from 3.5 years to more than 30 years, and all of the patients had very low self-esteem. Those who heard more than 1 voice were told to choose the one that was most dominant.
Pocket Therapist
Dr. Julian Leff shows examples of faces used in avatar therapy at RCPsych 2014.
During the sessions, the therapist sat in a separate room and played dual roles. He coached the participants on how to confront and talk with the avatars in his own voice, and he also voiced the avatars. All of the sessions were recorded and given to the participants on an MP3 recorder to play back if needed, to remind the patients how to confront and talk to the auditory hallucination if it reappeared.
“We told them: It’s like having a therapist in your pocket. Use it,” said Dr. Leff.
All of the avatars started out appearing very stern; they talked loudly and said horrible things to match what the patients had been reportedly experiencing. But after patients learned to talk back to the faces in more confident tones, the avatars began to “soften up” and discuss issues rationally and even offer advice.
Most of the participants who received avatar therapy went on after the study to be able to start new jobs. In addition, most reported that the voices went down to whispers, and 3 patients reported that the voices stopped completely.
The patient who confronted the red devil avatar reported that the voice had disappeared after 2 sessions. At the 3-month follow-up, he reported that the voice had returned, although at night only; he was told to go to bed earlier (to fight possible fatigue) and to use the MP3 player immediately beforehand. On all subsequent follow-ups, he reported that the voice was completely gone, and he has since gone on to work abroad.
Another patient who reported past experiences of abuse asked that his avatar be created wearing sunglasses because he could not bear to look at its eyes. During his sessions, Dr. Leff told him through the avatar that what had happened to the patient was not his fault. And at the end of 5 sessions, the phantom voice disappeared altogether.
Although 1 female patient reported that her phantom voice had not gone away, it had gotten much quieter. “When we asked her why, she said, ‘The voice now knows that if it talks to me, I’ll talk back,’ ” said Dr. Leff.
“These people are giving a face to an incredibly destructive force in their mind. Giving them control to create the avatar lets them control the situation and even make friends with it,” he added.
“The moment that a patient says something and the avatar responds differently than before, everything changes.”
In addition, there was a significant reduction in depression scores on the Calgary Depression Scale for Schizophrenia and in suicidal ideation for the avatar participants at the 3-month follow-up assessment.
A bigger study with a proposed sample size of 140 is currently under way and is “about a quarter of the way complete,” Dr. Leff reports. Of these patients, 70 will receive avatar therapy, and 70 will receive supportive counseling.
“In order for others to master this therapy, it is necessary to construct a treatment manual and this has now been completed, in preparation for the replication study,” write the investigators.
“One of its main aims is to determine whether clinicians working in a standard setting can be trained to achieve results comparable to those that emerged from the pilot study,” they add.
“Fascinating” New Therapy
“I think this is really exciting. It’s a fascinating, new form of therapy,” session moderator Sridevi Kalidindi, FRCPsych, consultant psychiatrist and clinical lead in rehabilitation at South London and Maudsley NHS Foundation Trust in the United Kingdom, told Medscape Medical News.
Dr. Sridevi Kalidindi
“I think it is a novel way of approaching these very challenging symptoms that people have. From the early results that have been presented, it provides hope for people that they may actually be able to improve from all of these symptoms. And we may be able to reduce their distress in quite a different way from anything we’ve ever done before.”
Dr. Kalidindi, who is also chair of the Rehabilitation Faculty for the Royal College of Psychiatrists, was not involved with this research.
She added that she will be watching this ongoing program “with great interest.”
“I was very enthused to learn that more research is going on with this particularly complex group,” said Dr. Kalidindi.
“This could be something for people who have perhaps not benefitted from other types of intervention. Overall, it’s fantastic.”
International Congress of the Royal College of Psychiatrists (RCPsych) 2014. Presented in 2 oral sessions on June 26, 2014.
Curling Ocean Wave in Red Room – Painting in Gouache
Not sure what to make of this painting, but I enjoyed doing it…What do you think? It is 8 by 12 inches, approximately, in gouache on Ampersand board (essentially gessoed masonite).